

Role of surgical resection for multiple hepatocellular carcinomas
- PMID: 23372359
- PMCID: PMC3554821
- DOI: 10.3748/wjg.v19.i3.366
Role of surgical resection for multiple hepatocellular carcinomas
Abstract
Aim: To clarify the role of surgical resection for multiple hepatocellular carcinomas (HCCs) compared to transarterial chemoembolization (TACE) and liver transplantation (LT).
Methods: Among the HCC patients who were managed at Yonsei University Health System between January 2003 and December 2008, 160 patients who met the following criteria were retrospectively enrolled: (1) two or three radiologically diagnosed HCCs; (2) no radiologic vascular invasion; (3) Child-Pugh class A; (4) main tumor smaller than 5 cm in diameter; and (5) platelet count greater than 50 000/mm(3). Long-term outcomes were compared among the following three treatment modalities: surgical resection or combined radiofrequency ablation (RFA) (n = 36), TACE (n = 107), and LT (n = 17). The survival curves were computed using the Kaplan-Meier method and compared with a log-rank test. To identify the patients who gained a survival benefit from surgical resection, we also investigated prognostic factors for survival following surgical resection. Multivariate analyses of the prognostic factors for survival were performed using the Cox proportional hazard model.
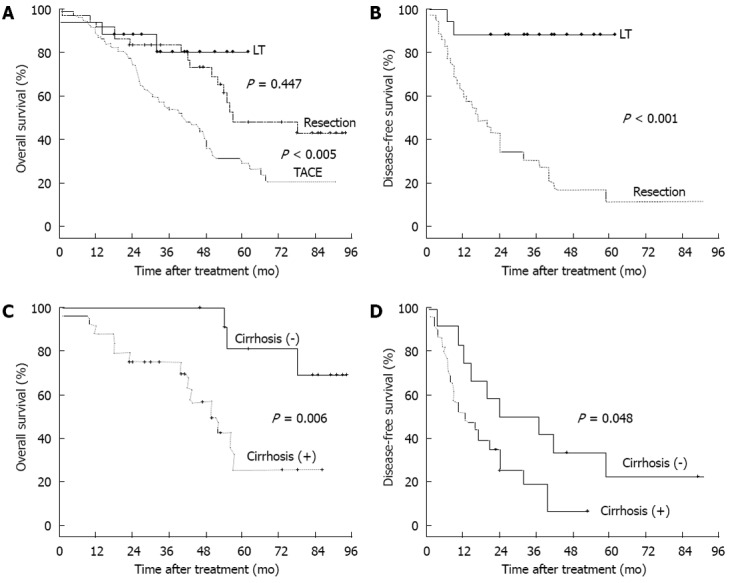
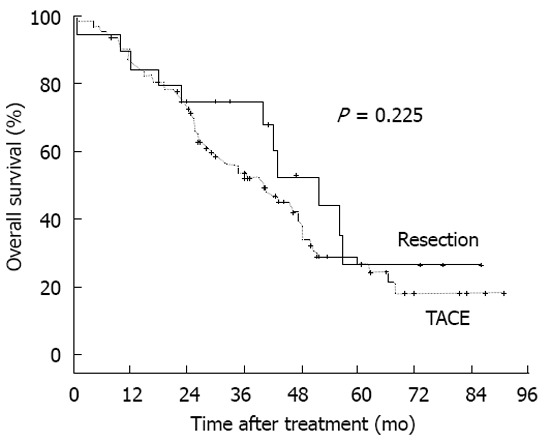
Results: The overall survival (OS) rate was significantly higher in the surgical resection group than in the TACE group (48.1% vs 28.9% at 5 years, P < 0.005). LT had the best OS rate, which was better than that of the surgical resection group, although the difference was not statistically significant (80.2% vs 48.1% at 5 years, P = 0.447). The disease-free survival rates were also significantly higher in the LT group than in the surgical resection group (88.2% vs 11.2% at 5 years, P < 0.001). Liver cirrhosis was the only significant prognostic factor for poor OS after surgical resection. Clinical liver cirrhosis rates were 55.6% (20/36) in the resection group and 93.5% (100/107) in the TACE group. There were 19 major and 17 minor resections. En bloc resection was performed in 23 patients, multi-site resection was performed in 5 patients, and combined resection with RFA was performed in 8 patients. In the TACE group, only 34 patients (31.8%) were recorded as having complete remission after primary TACE. Seventy-two patients (67.3%) were retreated with repeated TACE combined with other therapies. In patients who underwent surgical resection, the 16 patients who did not have cirrhosis had higher 5-year OS and disease-free survival rates than the 20 patients who had cirrhosis (80.8% vs 25.5% 5-year OS rate, P = 0.006; 22.2% vs 0% 5-year disease-free survival rate, P = 0.048). Surgical resection in the 20 patients who had cirrhosis did not provide any survival benefit when compared with TACE (25.5% vs 24.7% 5-year OS rate, P = 0.225). Twenty-nine of the 36 patients who underwent surgical resection experienced recurrence. Of the patients with cirrhosis, 80% (16/20) were within the Milan criteria at the time of recurrence after resection.
Conclusion: Among patients with two or three HCCs, no radiologic vascular invasion, and tumor diameters ≤ 5 cm, surgical resection is recommended only in those without cirrhosis.
Keywords: Chemoembolization; Cirrhosis; Hepatectomy; Hepatocellular carcinoma; Liver transplantation.
Figures
Similar articles
-
TACE Combined with HIFU Versus Surgical Resection for Single Hepatocellular Carcinoma with Child-Pugh B Cirrhosis in Overall Survival and Progression-Free Survival: A Retrospective Study.Technol Cancer Res Treat. 2021 Jan-Dec;20:15330338211060180. doi: 10.1177/15330338211060180. Technol Cancer Res Treat. 2021. PMID: 34855560 Free PMC article.
-
Partial hepatectomy vs. transcatheter arterial chemoembolization for resectable multiple hepatocellular carcinoma beyond Milan Criteria: a RCT.J Hepatol. 2014 Jul;61(1):82-8. doi: 10.1016/j.jhep.2014.03.012. Epub 2014 Mar 17. J Hepatol. 2014. PMID: 24650695 Clinical Trial.
-
[Experience of the treatment following downstaging of larger hepatocellular carcinomas by transcathetheter hepatic arterial chemoembolization in 58 patients].Zhonghua Yi Xue Za Zhi. 2011 Apr 12;91(14):950-5. Zhonghua Yi Xue Za Zhi. 2011. PMID: 21609544 Chinese.
-
Trans-arterial chemoembolization + radiofrequency ablation versus surgical resection in hepatocellular carcinoma - A meta-analysis.Eur J Surg Oncol. 2020 May;46(5):763-771. doi: 10.1016/j.ejso.2020.01.004. Epub 2020 Jan 7. Eur J Surg Oncol. 2020. PMID: 31937433 Review.
-
HCC: current surgical treatment concepts.Langenbecks Arch Surg. 2012 Jun;397(5):681-95. doi: 10.1007/s00423-012-0911-2. Langenbecks Arch Surg. 2012. PMID: 22290218 Review.
Cited by
-
Reduced red blood cell count predicts poor survival after surgery in patients with primary liver cancer.Medicine (Baltimore). 2015 Feb;94(8):e577. doi: 10.1097/MD.0000000000000577. Medicine (Baltimore). 2015. PMID: 25715259 Free PMC article.
-
Number of nodules, Child-Pugh status, margin positivity, and microvascular invasion, but not tumor size, are prognostic factors of survival after liver resection for multifocal hepatocellular carcinoma.J Gastrointest Surg. 2014 Aug;18(8):1477-85. doi: 10.1007/s11605-014-2542-0. Epub 2014 May 23. J Gastrointest Surg. 2014. PMID: 24855028
-
Surgical treatment of hepatocellular carcinoma: should resection be performed according to Barcelona Clinic Liver Cancer classification?Hepat Oncol. 2015 Jul;2(3):245-253. doi: 10.2217/hep.15.18. Epub 2015 Jul 30. Hepat Oncol. 2015. PMID: 30191006 Free PMC article. Review.
-
Dissecting the multinodular hepatocellular carcinoma subset: is there a survival benefit after hepatectomy?Updates Surg. 2019 Mar;71(1):57-66. doi: 10.1007/s13304-019-00626-3. Epub 2019 Mar 9. Updates Surg. 2019. PMID: 30852806
-
A deep learning-based clinical-radiomics model predicting the treatment response of immune checkpoint inhibitors (ICIs)-based conversion therapy in potentially convertible hepatocelluar carcinoma patients: a tumor marker prognostic study.Int J Surg. 2025 May 1;111(5):3342-3355. doi: 10.1097/JS9.0000000000002322. Int J Surg. 2025. PMID: 40085751 Free PMC article.
References
-
- Wu CC, Cheng SB, Ho WM, Chen JT, Liu TJ, P’eng FK. Liver resection for hepatocellular carcinoma in patients with cirrhosis. Br J Surg. 2005;92:348–355. - PubMed
-
- Esnaola NF, Mirza N, Lauwers GY, Ikai I, Regimbeau JM, Belghiti J, Yamaoka Y, Curley SA, Ellis LM, Nagorney DM, et al. Comparison of clinicopathologic characteristics and outcomes after resection in patients with hepatocellular carcinoma treated in the United States, France, and Japan. Ann Surg. 2003;238:711–719. - PMC - PubMed
-
- Bruix J, Sherman M. Management of hepatocellular carcinoma. Hepatology. 2005;42:1208–1236. - PubMed
-
- Bruix J, Sherman M, Llovet JM, Beaugrand M, Lencioni R, Burroughs AK, Christensen E, Pagliaro L, Colombo M, Rodés J. Clinical management of hepatocellular carcinoma. Conclusions of the Barcelona-2000 EASL conference. European Association for the Study of the Liver. J Hepatol. 2001;35:421–430. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
