

Lateral abdominal wall reconstruction
- PMID: 23372458
- PMCID: PMC3348741
- DOI: 10.1055/s-0032-1302465
Lateral abdominal wall reconstruction
Abstract
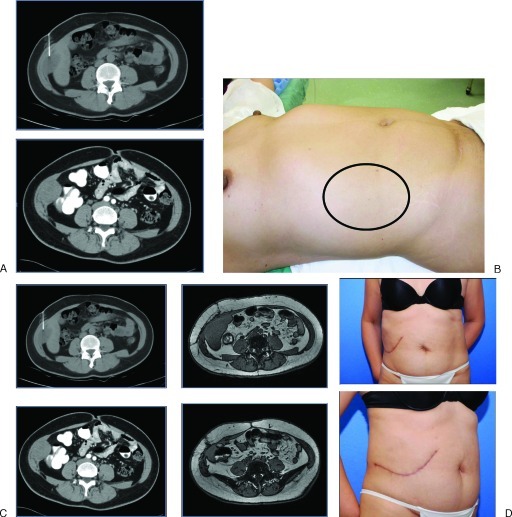
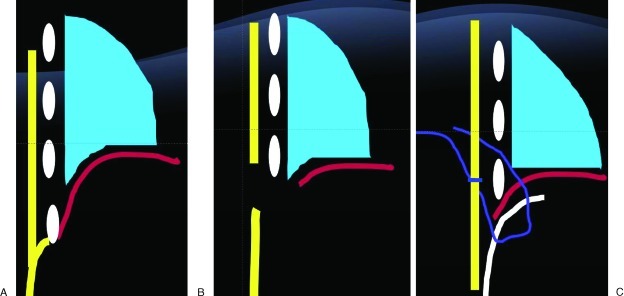
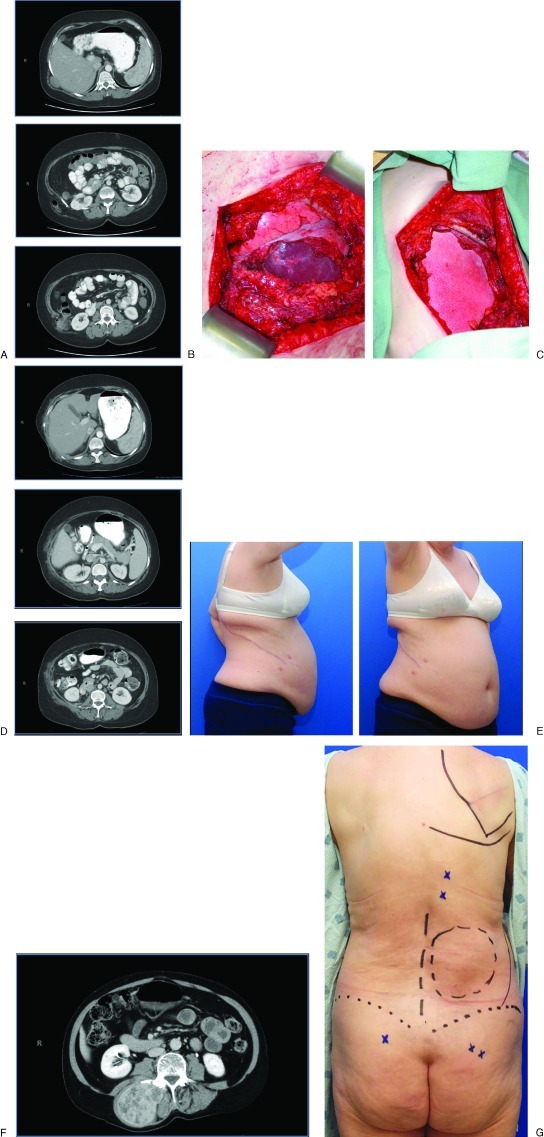
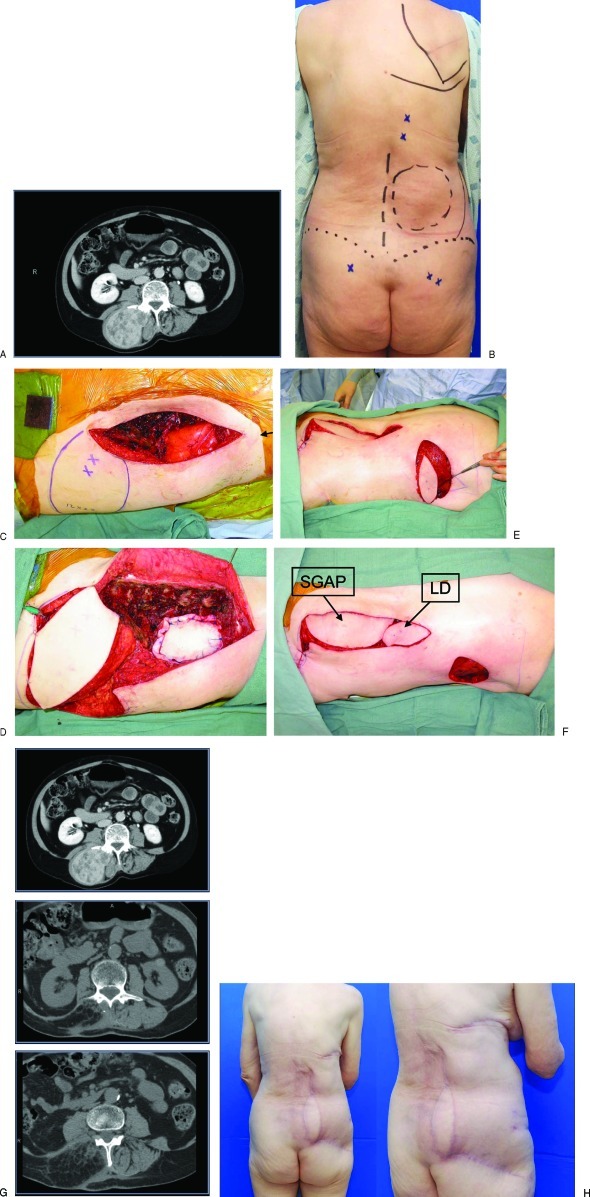
Lateral abdominal wall (LAW) defects can manifest as a flank hernias, myofascial laxity/bulges, or full-thickness defects. These defects are quite different from those in the anterior abdominal wall defects and the complexity and limited surgical options make repairing the LAW a challenge for the reconstructive surgeon. LAW reconstruction requires an understanding of the anatomy, physiologic forces, and the impact of deinnervation injury to design and perform successful reconstructions of hernia, bulge, and full-thickness defects. Reconstructive strategies must be tailored to address the inguinal ligament, retroperitoneum, chest wall, and diaphragm. Operative technique must focus on stabilization of the LAW to nonyielding points of fixation at the anatomic borders of the LAW far beyond the musculofascial borders of the defect itself. Thus, hernias, bulges, and full-thickness defects are approached in a similar fashion. Mesh reinforcement is uniformly required in lateral abdominal wall reconstruction. Inlay mesh placement with overlying myofascial coverage is preferred as a first-line option as is the case in anterior abdominal wall reconstruction. However, interposition bridging repairs are often performed as the surrounding myofascial tissue precludes a dual layered closure. The decision to place bioprosthetic or prosthetic mesh depends on surgeon preference, patient comorbidities, and clinical factors of the repair. Regardless of mesh type, the overlying soft tissue must provide stable cutaneous coverage and obliteration of dead space. In cases where the fasciocutaneous flaps surrounding the defect are inadequate for closure, regional pedicled flaps or free flaps are recruited to achieve stable soft tissue coverage.
Keywords: biologic mesh; bioprosthetic mesh; bulge; component separation; hernia; lateral abdominal wall reconstruction.
Figures
Similar articles
-
Minimally invasive component separation with inlay bioprosthetic mesh (MICSIB) for complex abdominal wall reconstruction.Plast Reconstr Surg. 2011 Sep;128(3):698-709. doi: 10.1097/PRS.0b013e318221dcce. Plast Reconstr Surg. 2011. PMID: 21572378
-
A challenge in soft tissue reconstruction: The use of pedicled anterolateral thigh fasciocutaneous flap and gluteal fasciocutaneous rotational flap in reconstructing a huge full thickness lateral trunk defect.Ann Med Surg (Lond). 2021 Oct 9;71:102933. doi: 10.1016/j.amsu.2021.102933. eCollection 2021 Nov. Ann Med Surg (Lond). 2021. PMID: 34745600 Free PMC article.
-
An Evidence-Based Model for the Successful Treatment of Flank and Lateral Abdominal Wall Hernias.Plast Reconstr Surg. 2015 Aug;136(2):377-385. doi: 10.1097/PRS.0000000000001432. Plast Reconstr Surg. 2015. PMID: 25946603
-
Lateral Abdominal Wall Reconstruction.Semin Plast Surg. 2018 Aug;32(3):141-146. doi: 10.1055/s-0038-1666801. Epub 2018 Jul 24. Semin Plast Surg. 2018. PMID: 30046290 Free PMC article. Review.
-
'Sandwich' technique in the treatment of large and complex incisional hernias.ANZ J Surg. 2016 May;86(5):343-7. doi: 10.1111/ans.13285. Epub 2015 Sep 1. ANZ J Surg. 2016. PMID: 26331991 Review.
Cited by
-
Peritoneal flap hernioplasty for repair of incisional hernias after orthotopic liver transplantation.Hernia. 2022 Apr;26(2):481-487. doi: 10.1007/s10029-021-02409-5. Epub 2021 Apr 22. Hernia. 2022. PMID: 33884521 Free PMC article.
-
Athletic injuries of the lateral abdominal wall: review of anatomy and MR imaging appearance.Skeletal Radiol. 2016 Feb;45(2):155-62. doi: 10.1007/s00256-015-2261-y. Epub 2015 Oct 9. Skeletal Radiol. 2016. PMID: 26450606 Review.
-
MIS retromuscular repair of lateral incisional hernia: technological deliberations and short-term outcome.Hernia. 2022 Oct;26(5):1325-1336. doi: 10.1007/s10029-022-02671-1. Epub 2022 Sep 10. Hernia. 2022. PMID: 36088435
-
Management of lateral abdominal hernias.Hernia. 2020 Apr;24(2):353-358. doi: 10.1007/s10029-020-02126-5. Epub 2020 Feb 12. Hernia. 2020. PMID: 32052297
-
Repair of giant subcostal hernia using porcine acellular dermal matrix (Strattice™) with bone anchors and pedicled omental flap coverage: a case report.J Med Case Rep. 2013 Nov 11;7:258. doi: 10.1186/1752-1947-7-258. J Med Case Rep. 2013. PMID: 24215723 Free PMC article.
References
-
- Bender J S, Dennis R W, Albrecht R M. Traumatic flank hernias: acute and chronic management. Am J Surg. 2008;195(3):414–417, discussion 417. - PubMed
-
- Burt B M, Afifi H Y, Wantz G E, Barie P S. Traumatic lumbar hernia: report of cases and comprehensive review of the literature. J Trauma. 2004;57(6):1361–1370. - PubMed
-
- Fakhry S M, Azizkhan R G. Observations and current operative management of congenital lumbar hernias during infancy. Surg Gynecol Obstet. 1991;172(6):475–479. - PubMed
-
- Chatterjee S, Nam R, Fleshner N, Klotz L. Permanent flank bulge is a consequence of flank incision for radical nephrectomy in one half of patients. Urol Oncol. 2004;22(1):36–39. - PubMed
-
- Matsen S L, Krosnick T A, Roseborough G S. et al.Preoperative and intraoperative determinants of incisional bulge following retroperitoneal aortic repair. Ann Vasc Surg. 2006;20(2):183–187. - PubMed
