

Understanding the potential impact of a combination HIV prevention intervention in a hyper-endemic community
- PMID: 23372738
- PMCID: PMC3553021
- DOI: 10.1371/journal.pone.0054575
Understanding the potential impact of a combination HIV prevention intervention in a hyper-endemic community
Abstract
Objectives: Despite demonstrating only partial efficacy in preventing new infections, available HIV prevention interventions could offer a powerful strategy when combined. In anticipation of combination HIV prevention programs and research studies we estimated the population-level impact of combining effective scalable interventions at high population coverage, determined the factors that influence this impact, and estimated the synergy between the components.
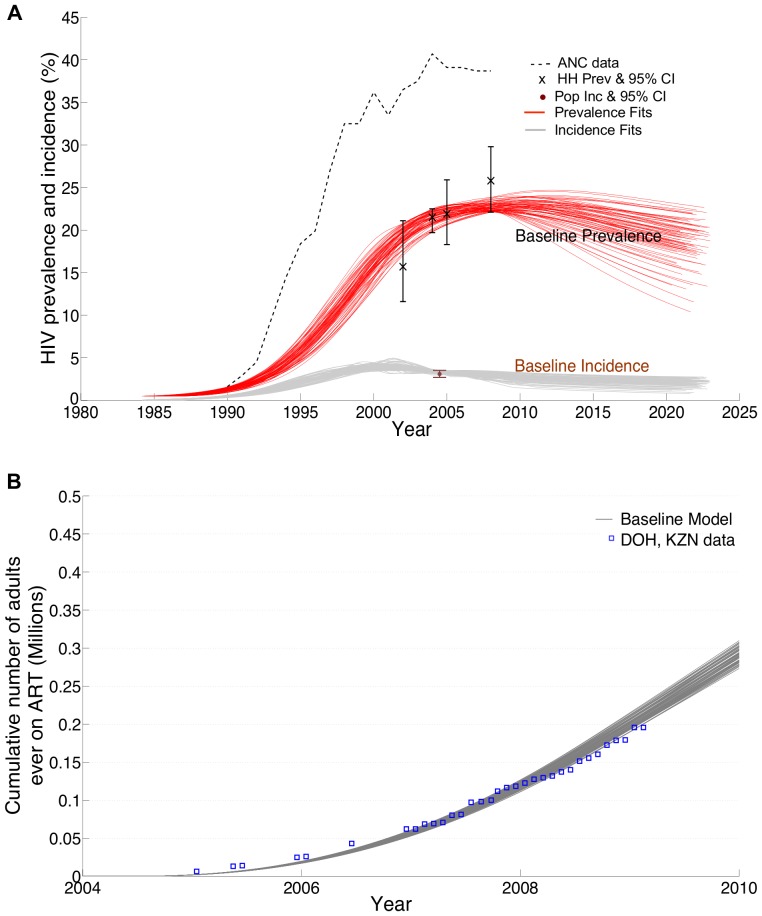
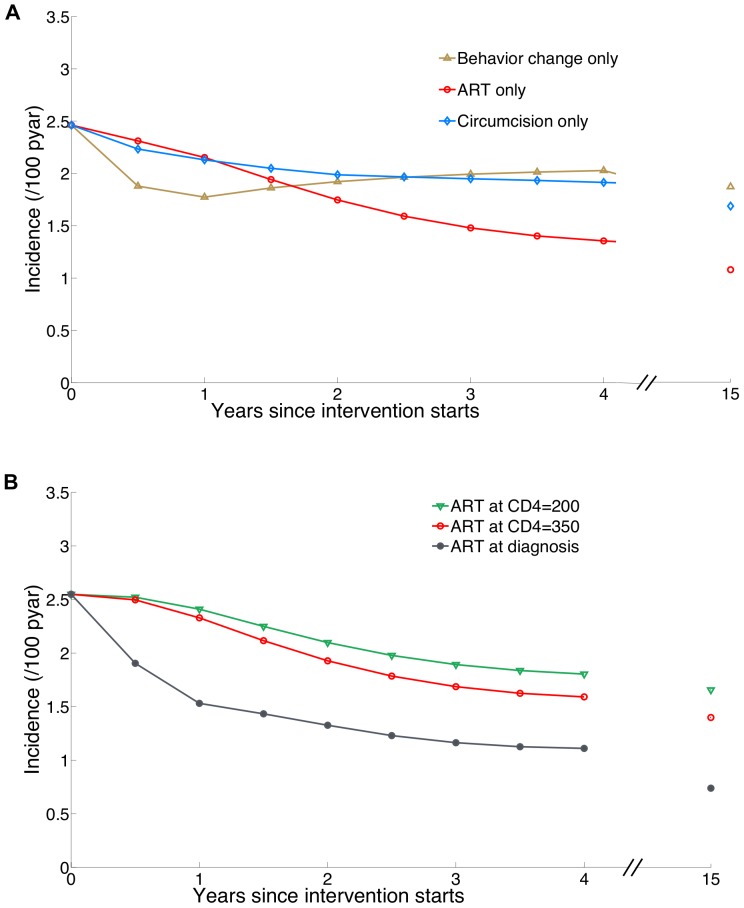
Methods: We used a mathematical model to investigate the effect on HIV incidence of a combination HIV prevention intervention comprised of high coverage of HIV testing and counselling, risk reduction following HIV diagnosis, male circumcision for HIV-uninfected men, and antiretroviral therapy (ART) for HIV-infected persons. The model was calibrated to data for KwaZulu-Natal, South Africa, where adult HIV prevalence is approximately 23%.
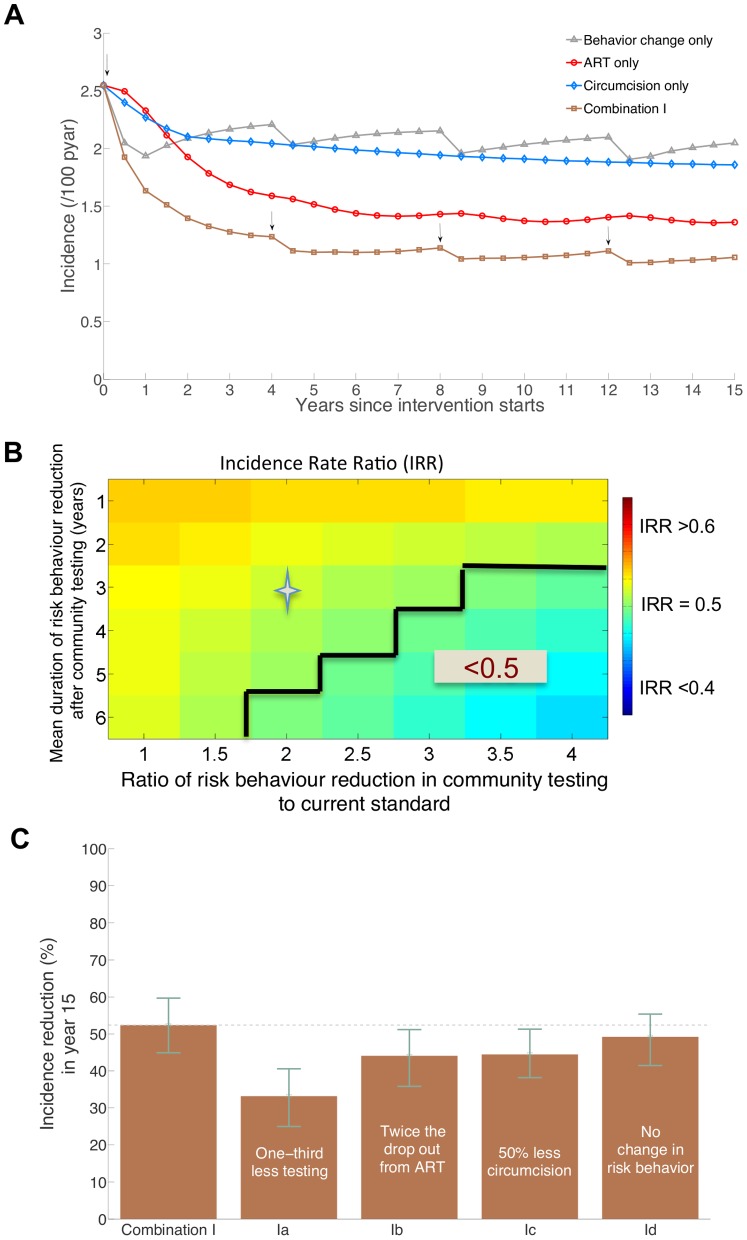
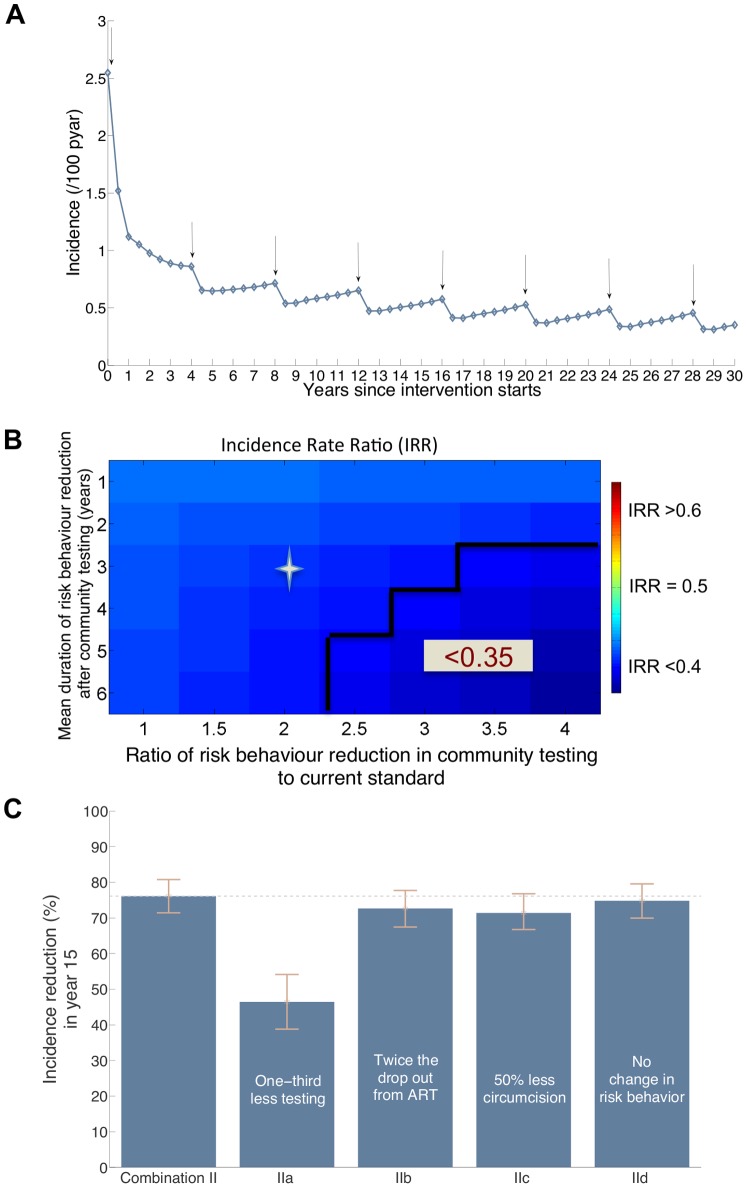
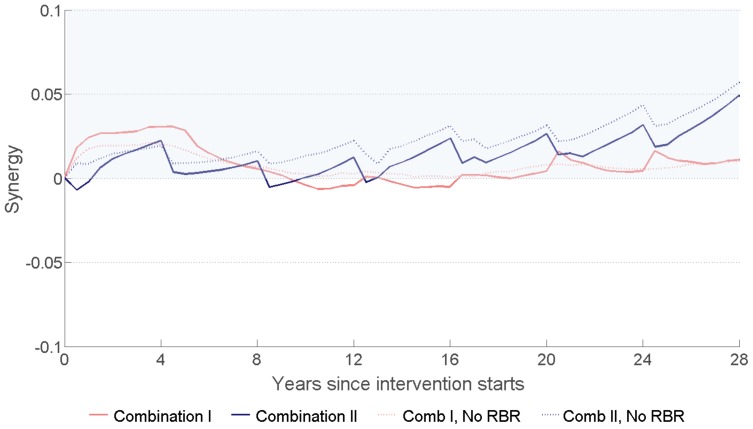
Results: Compared to current levels of HIV testing, circumcision, and ART, the combined intervention with ART initiation according to current guidelines could reduce HIV incidence by 47%, from 2.3 new infections per 100 person-years (pyar) to 1.2 per 100 pyar within 4 years and by almost 60%, to 1 per 100 pyar, after 25 years. Short-term impact is driven primarily by uptake of testing and reductions in risk behaviour following testing while long-term effects are driven by periodic HIV testing and retention in ART programs. If the combination prevention program incorporated HIV treatment upon diagnosis, incidence could be reduced by 63% after 4 years and by 76% (to about 0.5 per 100 pyar) after 15 years. The full impact of the combination interventions accrues over 10-15 years. Synergy is demonstrated between the intervention components.
Conclusion: High coverage combination of evidence-based strategies could generate substantial reductions in population HIV incidence in an African generalized HIV epidemic setting. The full impact could be underestimated by the short assessment duration of typical evaluations.
Conflict of interest statement
Figures
References
-
- Bailey RC, Moses S, Parker CB, Agot K, Maclean I, et al. (2007) Male circumcision for HIV prevention in young men in Kisumu, Kenya: a randomised controlled trial. The Lancet 369: 643–656. - PubMed
-
- Gray RH, Kigozi G, Serwadda D, Makumbi F, Watya S, et al. (2007) Male circumcision for HIV prevention in men in Rakai, Uganda: a randomised trial. The Lancet 369: 657–666. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
