

Dorsal paddle leads implant for spinal cord stimulation through laminotomy with midline structures preservation
- PMID: 23372980
- PMCID: PMC3551524
- DOI: 10.4103/2152-7806.105275
Dorsal paddle leads implant for spinal cord stimulation through laminotomy with midline structures preservation
Abstract
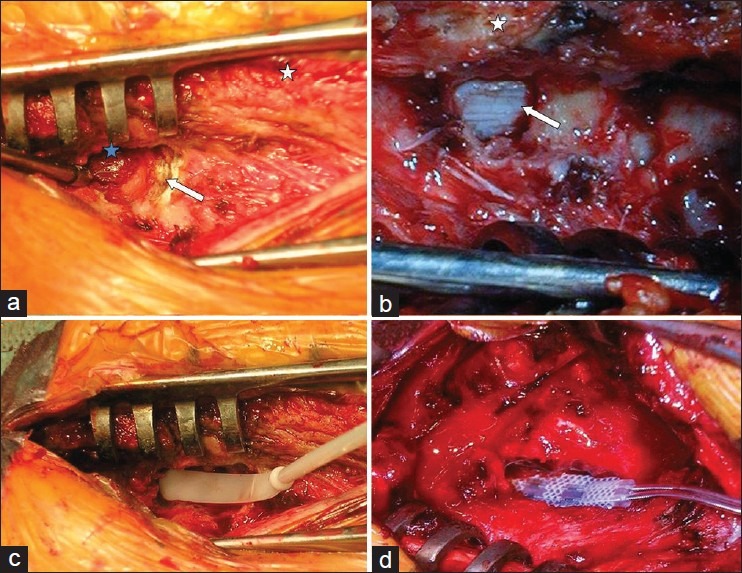
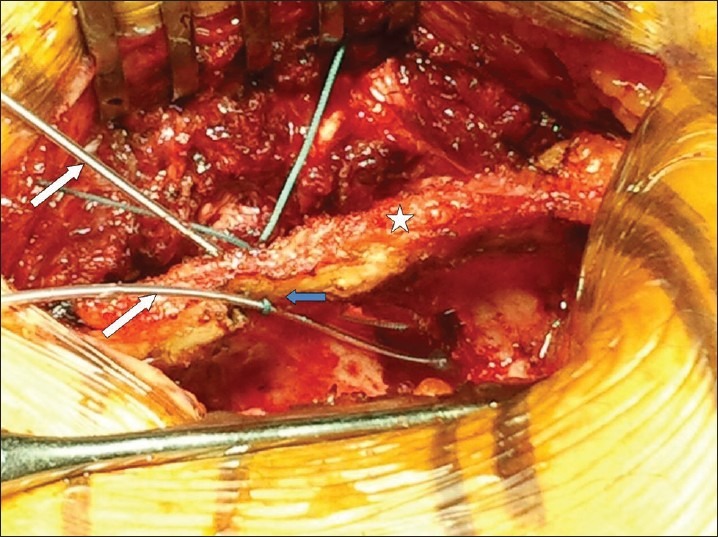
Background: Pain relief obtained with spinal cord stimulation (SCS) in failed back surgery syndrome (FBSS) has been shown to be more effective with paddle leads than with percutaneous catheters. A laminectomy is generally required to implant the paddles, but the surgical approach may lead to iatrogenic spinal instability in flexion. In contrast, clinical and experimental data showed that a laminotomy performed through flavectomy and minimal resection of inferior and superior lamina with preservation of the midline ligamentous structures allowed to prevent iatrogenic instability. Aim of the study was to assess degree of instability and pain level in patients operated for SCS through laminectomy or laminotomy with midline structures integrity. The surgical technique is described and our preliminary results are discussed.
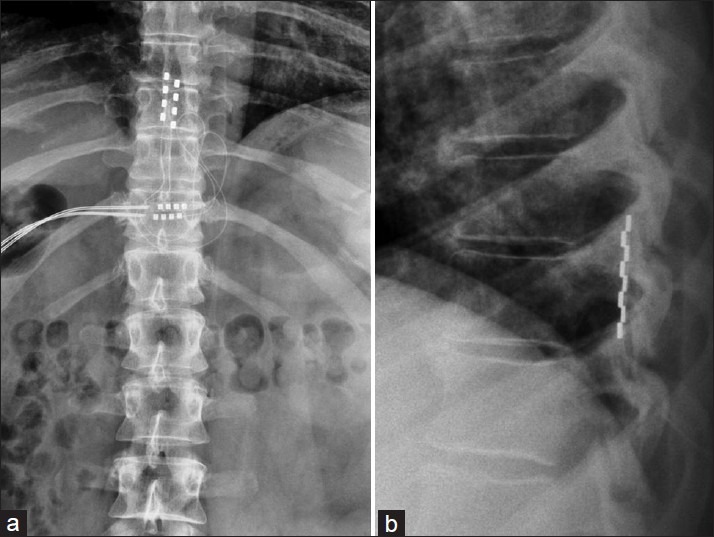
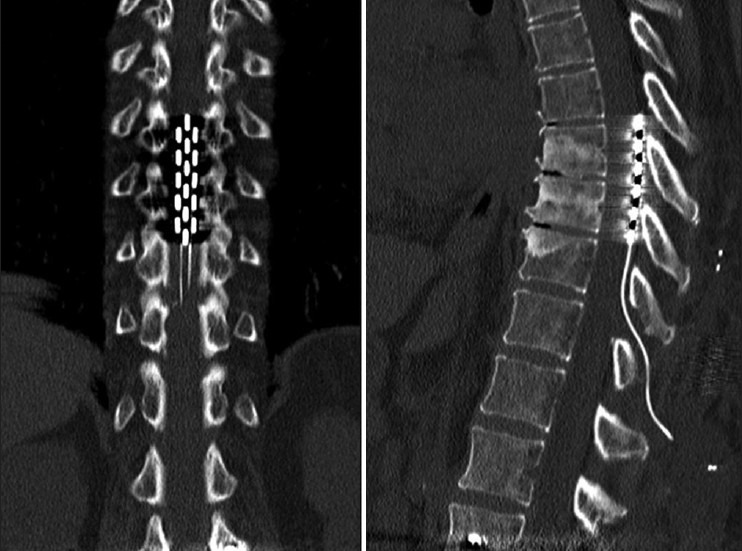
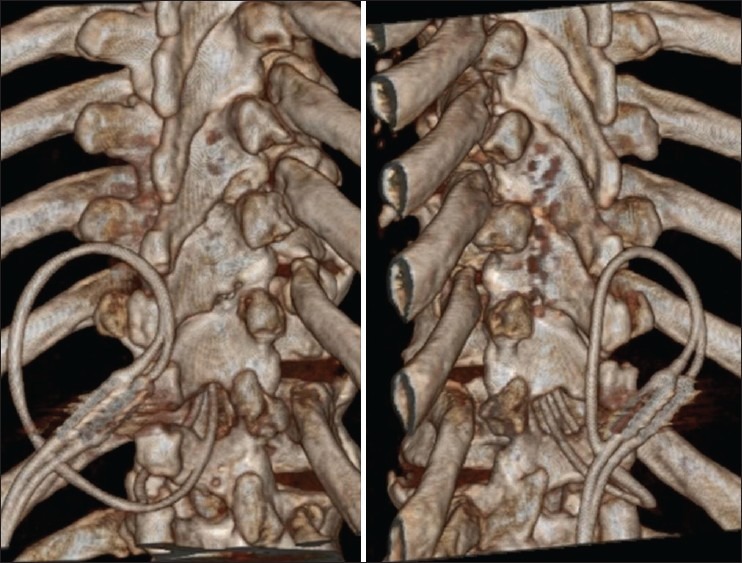
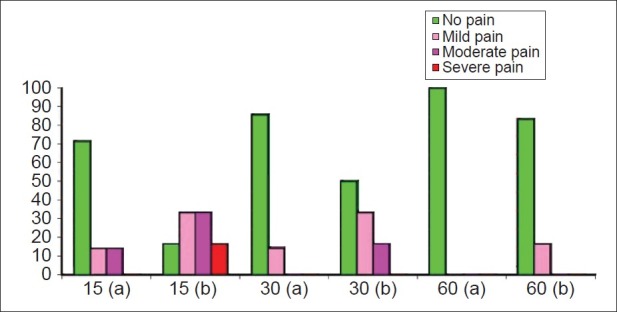
Methods: Nineteen patients with FBSS underwent SCS, 12 through laminectomy and 7 through uni- or bilateral interlaminotomy with supraspinous ligament preservation. Postoperative local pain was evaluated at 15, 30, and 60 days. Static and dynamic X-rays were performed after 2 months.
Results: The techniques allowed implanting the paddle leads in all cases. No intraoperative complications occurred. Local pain was higher and recovery time was longer in patients with laminectomy. We did not observe radiological signs of postoperative iatrogenic vertebral instability. Nevertheless, two patients who underwent laminectomy showed persistence of local pain after 2 months probably due to pathologic compensatory stability provided by the paraspinal musculature.
Conclusions: The laminotomy is a minimally invasive approach that ensures rapid recovery after surgery, spinal functional integrity, and complete reversibility. Further studies are needed to confirm our preliminary results.
Keywords: Failed back surgery syndrome; laminotomy; paddle lead; spinal cord stimulation minimally invasive technique.
Figures
Similar articles
-
Predictors of Skip Laminotomy for Placement of Paddle Leads for Spinal Cord Stimulation.Neuromodulation. 2024 Jan;27(1):183-187. doi: 10.1016/j.neurom.2023.07.011. Epub 2023 Aug 24. Neuromodulation. 2024. PMID: 37632516
-
Percutaneous implanted paddle lead for spinal cord stimulation: technical considerations and long-term follow-up.Neuromodulation. 2012 Jul;15(4):402-7. doi: 10.1111/j.1525-1403.2012.00473.x. Epub 2012 Jun 1. Neuromodulation. 2012. PMID: 22672364
-
Placement of Surgical Spinal Cord Stimulation Leads Using Spinal Process Splitting Laminotomy: Technical Note.World Neurosurg. 2021 Nov;155:109-114. doi: 10.1016/j.wneu.2021.07.146. Epub 2021 Aug 8. World Neurosurg. 2021. PMID: 34375778
-
Spinal cord stimulation with implanted epidural paddle lead relieves chronic axial low back pain.J Pain Res. 2014 Aug 12;7:465-70. doi: 10.2147/JPR.S66414. eCollection 2014. J Pain Res. 2014. PMID: 25143753 Free PMC article. Review.
-
Development of a Modified Bayonet Forceps for Improving Steerability of Paddle Lead Electrodes During Spinal Cord Stimulator Surgery: A Technical Note.Oper Neurosurg. 2023 Sep 1;25(3):285-291. doi: 10.1227/ons.0000000000000779. Epub 2023 Jun 27. Oper Neurosurg. 2023. PMID: 37366619 Review.
Cited by
-
A case study of percutaneous epidural stimulation to enable motor control in two men after spinal cord injury.Nat Commun. 2023 Apr 12;14(1):2064. doi: 10.1038/s41467-023-37845-7. Nat Commun. 2023. PMID: 37045845 Free PMC article. Clinical Trial.
-
Efficacy analysis of two surgical treatments for thoracic and lumbar intraspinal tumours.BMC Surg. 2019 Sep 10;19(1):131. doi: 10.1186/s12893-019-0602-9. BMC Surg. 2019. PMID: 31500614 Free PMC article.
References
-
- Abeloos L, De Witte O, Riquet R, Tuna T, Mathieu N. Long-term outcome of patients treated with spinal cord stimulation for therapeutically refractory failed back surgery syndrome: A retrospective study. Neurochirurgie. 2011;57:114–9. - PubMed
-
- Ball PA, Fanciullo GJ. Pont de dolor: A dual laminotomy technique for placing and securing an electrode in the epidural space and comments about anatomic variation that may complicate spinal cord stimulator electrode placement. Neuromodulation. 2003;6:92–4. - PubMed
-
- Barolat G. Epidural spinal cord stimulation with a multiple electrode paddle leads is effective in treating intractable low back pain. Neuromodulation. 2001;4:59–66. - PubMed
-
- Barolat G, Sharan A, Ong J. Spinal cord stimulation for back pain. In: Simpson BA, editor. Electrical stimulation and the relief of pain. 1st ed. Vol. 15. Elsevier, Pain Res and Clin Man; 2003. pp. 79–86.
-
- Cameron T. Safety and efficacy of spinal cord stimulation for the treatment of chronic pain: A 20-year literature review. J Neurosurg. 2004;100:254–67. - PubMed
LinkOut - more resources
Full Text Sources
