

Increasing incidence of nutritional rickets: a population-based study in Olmsted County, Minnesota
- PMID: 23374621
- PMCID: PMC3612965
- DOI: 10.1016/j.mayocp.2012.10.018
Increasing incidence of nutritional rickets: a population-based study in Olmsted County, Minnesota
Abstract
Objective: To determine temporal trends in incidence and risk factors of nutritional rickets in a community-based population.
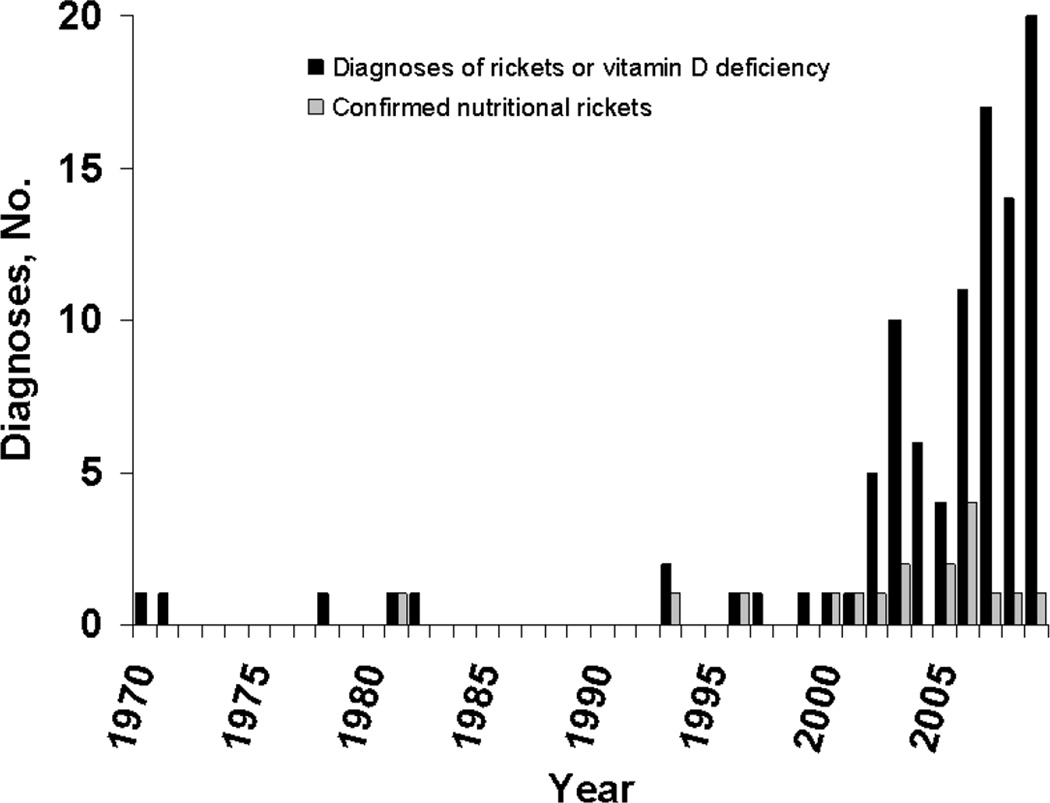
Patients and methods: Rochester Epidemiology Project data were used to identify all children (aged <18 years) residing in Olmsted County, Minnesota, between January 1, 1970, and December 31, 2009, with diagnostic codes corresponding to rickets, vitamin D deficiency, hypovitaminosis D, rachitis, osteomalacia, genu varum, genu valgum, craniotabes, hypocalcemia, hypocalcemic seizure, and tetany. Record abstraction was performed to select individuals with radiographic confirmation of rickets. Age- and sex-matched controls were identified for the evaluation of risk factors. The main outcome measure was radiographic evidence of rickets without identifiable inherited, genetic, or nonnutritional causes. Incidence rates were calculated using Rochester Epidemiology Project census data.
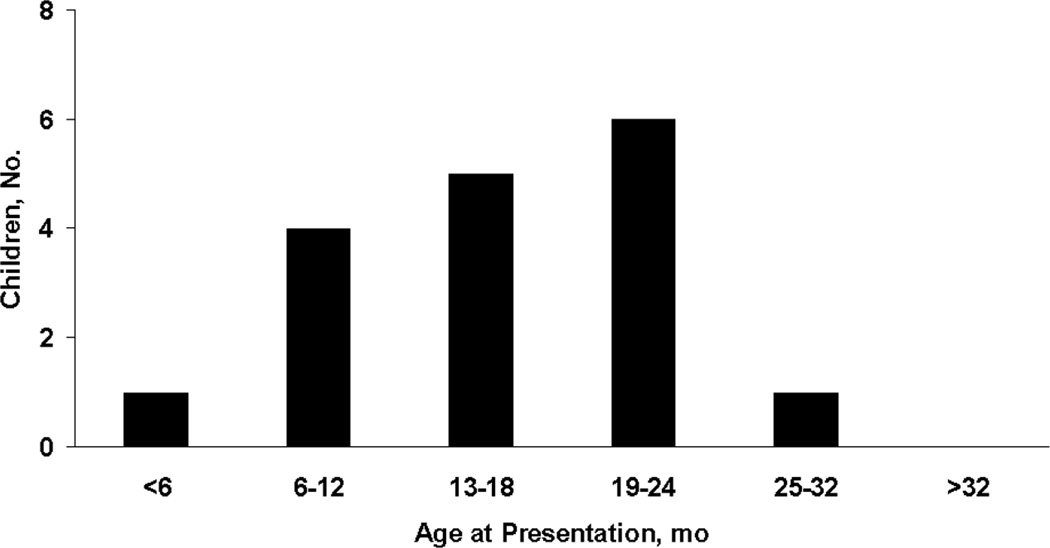
Results: Of 768 children with eligible diagnostic codes, 23 had radiographic evidence of rickets; of these, 17 children had nutritional rickets. All 17 children were younger than 3 years, and 13 (76%) were of nonwhite race/ethnicity. Clinical presentation included poor growth (n=12), leg deformity (n=8), motor delay (n=5), leg pain (n=3), weakness (n=3), and hypocalcemia or tetany (n=2). The incidence of nutritional rickets in children younger than 3 years was 0, 2.2, 3.7, and 24.1 per 100,000 for the decades beginning in 1970, 1980, 1990, and 2000, respectively (P=.003 for incidence trend). Nutritional rickets was associated with black race, breast-feeding, low birth weight, and stunted growth (P<.05 for all). Four of 13 patients (31%) who underwent 25-hydroxyvitamin D testing had values less than 10 ng/mL.
Conclusion: Nutritional rickets remains rare, but its incidence has dramatically increased since 2000. Not all cases of rickets can be attributed to vitamin D deficiency.
Copyright © 2013 Mayo Foundation for Medical Education and Research. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Pettifor JM. Nutritional rickets: deficiency of vitamin D, calcium, or both? Am J Clin Nutr. 2004;80(6 Suppl):1725S–1729S. - PubMed
-
- Weisberg P, Scanlon KS, Li R, Cogswell ME. Nutritional rickets among children in the United States: review of cases reported between 1986 and 2003. Am J Clin Nutr. 2004;80(6 Suppl):1697S–1705S. - PubMed
-
- Tomashek KM, Nesby S, Scanlon KS, et al. Nutritional rickets in Georgia. Pediatrics. 2001;107(4):E45. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
