

Surgical inflammatory stress: the embryo takes hold of the reins again
- PMID: 23374964
- PMCID: PMC3577641
- DOI: 10.1186/1742-4682-10-6
Surgical inflammatory stress: the embryo takes hold of the reins again
Abstract
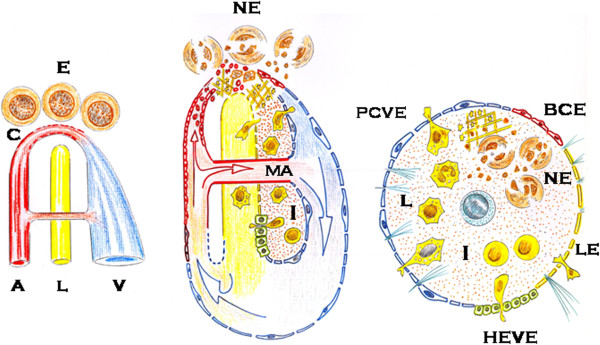
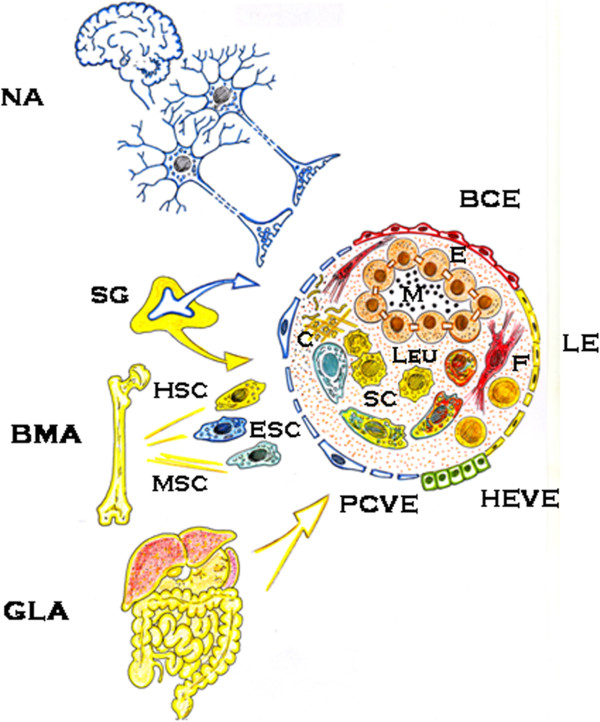
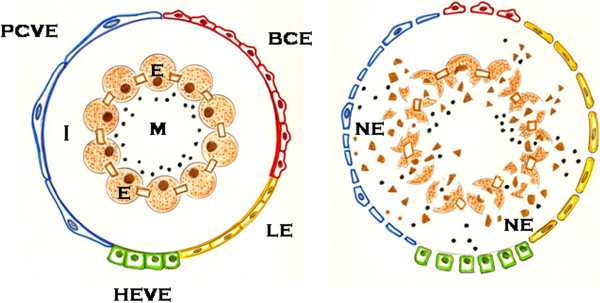
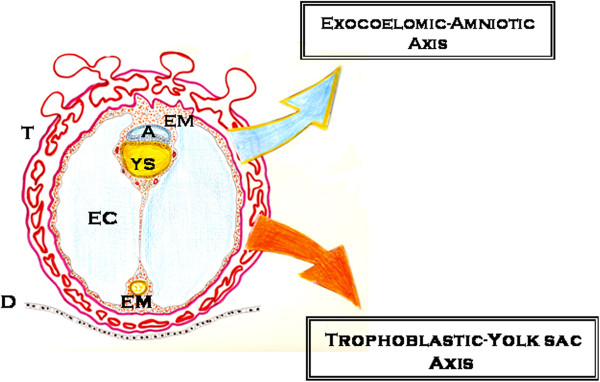
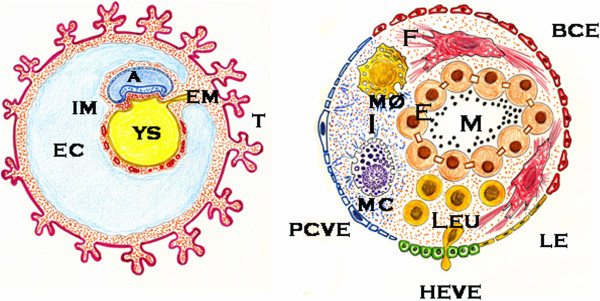
The surgical inflammatory response can be a type of high-grade acute stress response associated with an increasingly complex trophic functional system for using oxygen. This systemic neuro-immune-endocrine response seems to induce the re-expression of 2 extraembryonic-like functional axes, i.e. coelomic-amniotic and trophoblastic-yolk-sac-related, within injured tissues and organs, thus favoring their re-development. Accordingly, through the up-regulation of two systemic inflammatory phenotypes, i.e. neurogenic and immune-related, a gestational-like response using embryonic functions would be induced in the patient's injured tissues and organs, which would therefore result in their repair. Here we establish a comparison between the pathophysiological mechanisms that are produced during the inflammatory response and the physiological mechanisms that are expressed during early embryonic development. In this way, surgical inflammation could be a high-grade stress response whose pathophysiological mechanisms would be based on the recapitulation of ontogenic and phylogenetic-related functions. Thus, the ultimate objective of surgical inflammation, as a gestational process, is creating new tissues/organs for repairing the injured ones. Since surgical inflammation and early embryonic development share common production mechanisms, the factors that hamper the wound healing reaction in surgical patients could be similar to those that impair the gestational process.
Figures
Similar articles
-
The gestational power of mast cells in the injured tissue.Inflamm Res. 2018 Feb;67(2):111-116. doi: 10.1007/s00011-017-1108-5. Epub 2017 Nov 3. Inflamm Res. 2018. PMID: 29101413 Review.
-
Embrionary way to create a fatty liver in portal hypertension.World J Gastrointest Pathophysiol. 2017 May 15;8(2):39-50. doi: 10.4291/wjgp.v8.i2.39. World J Gastrointest Pathophysiol. 2017. PMID: 28573066 Free PMC article. Review.
-
The wound-healing response and upregulated embryonic mechanisms: brothers-in-arms forever.Exp Dermatol. 2012 Jul;21(7):497-503. doi: 10.1111/j.1600-0625.2012.01525.x. Exp Dermatol. 2012. PMID: 22716244
-
Surgical inflammation: a pathophysiological rainbow.J Transl Med. 2009 Mar 23;7:19. doi: 10.1186/1479-5876-7-19. J Transl Med. 2009. PMID: 19309494 Free PMC article. Review.
-
Pathological axes of wound repair: gastrulation revisited.Theor Biol Med Model. 2010 Sep 14;7:37. doi: 10.1186/1742-4682-7-37. Theor Biol Med Model. 2010. PMID: 20840764 Free PMC article.
Cited by
-
The gestational power of mast cells in the injured tissue.Inflamm Res. 2018 Feb;67(2):111-116. doi: 10.1007/s00011-017-1108-5. Epub 2017 Nov 3. Inflamm Res. 2018. PMID: 29101413 Review.
-
Establishment and validation of a predictive model for mortality within 30 days in patients with sepsis-induced blood pressure drop: A retrospective analysis.PLoS One. 2021 May 20;16(5):e0252009. doi: 10.1371/journal.pone.0252009. eCollection 2021. PLoS One. 2021. PMID: 34015023 Free PMC article.
-
Embrionary way to create a fatty liver in portal hypertension.World J Gastrointest Pathophysiol. 2017 May 15;8(2):39-50. doi: 10.4291/wjgp.v8.i2.39. World J Gastrointest Pathophysiol. 2017. PMID: 28573066 Free PMC article. Review.
-
Electroacupuncture Alleviates Surgical Trauma-Induced Hypothalamus Pituitary Adrenal Axis Hyperactivity Via microRNA-142.Front Mol Neurosci. 2017 Sep 27;10:308. doi: 10.3389/fnmol.2017.00308. eCollection 2017. Front Mol Neurosci. 2017. PMID: 29021740 Free PMC article.
-
Wound healing reaction: A switch from gestation to senescence.World J Exp Med. 2014 May 20;4(2):16-26. doi: 10.5493/wjem.v4.i2.16. eCollection 2014 May 20. World J Exp Med. 2014. PMID: 24977118 Free PMC article. Review.
References
-
- Selye H. A syndrome produced by diverse noxious agents. Nature. 1936;138:32. - PubMed
-
- Selye H. In: The stress of life. Revised edition. Selye H, editor. Mc Graw-Hill Book Co, New York; 1978. Stress and inflammation; pp. 129–143.
-
- Van de Kar LD, Richarson-Morton KD, Rittenhouse PA. In: Stress Revisited. 1. Neuroendocrinology of stress. Jasmin G, Cantin M, editor. Karger, Basel; 1991. Stress: Neuroendocrine and pharmacological mechanisms; pp. 133–173. - PubMed
-
- Laborit H. In: Stress revisited. 2. Systemic effects of stress. Methods and achievements in Experimental Pathology. Jasmin G, Proschek L, editor. Karger, Basel; 1991. The major mechanisms of stress; pp. 1–26. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
