

Regional intensity of vascular care and lower extremity amputation rates
- PMID: 23375611
- PMCID: PMC3660510
- DOI: 10.1016/j.jvs.2012.11.068
Regional intensity of vascular care and lower extremity amputation rates
Abstract
Objective: Because patient-level differences do not fully explain the variation in lower extremity amputation rates across the United States, we hypothesized that variation in intensity of vascular care may also affect regional rates of amputation and examined the relationship between the intensity of vascular care and the population-based rate of major lower extremity amputation (above-knee or below-knee) from vascular disease.
Methods: Intensity of vascular care was defined as the proportion of Medicare patients who underwent any vascular procedure in the year before amputation, calculated at the regional level (2003 to 2006), using the 306 hospital referral regions in the Dartmouth Atlas of Healthcare. The relationship between intensity of vascular care and major amputation rate, at the regional level, was examined between 2007 and 2009.
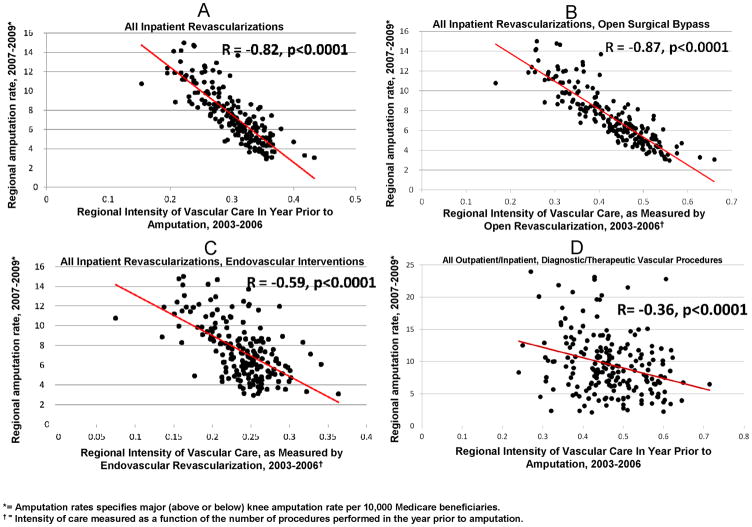
Results: Amputation rates varied widely by region, from one to 27 per 10,000 Medicare patients. Compared with regions in the lowest quintile of amputation rate, patients in the highest quintile were commonly African American (50% vs 13%) and diabetic (38% vs 31%). Intensity of vascular care also varied across regions: <35% of patients underwent revascularization in the lowest quintile of intensity, whereas nearly 60% underwent revascularization in the highest quintile. Overall, an inverse correlation was found between intensity of vascular care and the amputation rate, ranging from R = -0.36 for outpatient diagnostic and therapeutic procedures to R = -0.87 for inpatient surgical revascularizations. Analyses adjusting for patient characteristics and socioeconomic status found patients in high-intensity vascular care regions were significantly less likely to undergo amputation without an antecedent attempt at revascularization (odds ratio, 0.37; 95% confidence interval, 0.34-0.37; P < .001).
Conclusions: The intensity of vascular care provided to patients at risk for amputation varies, and regions with the most intensive vascular care have the lowest amputation rate, although the observational nature of these associations do not impart causality. High-risk patients, especially African American diabetic patients residing in low-intensity vascular care regions, represent an important target for systematic efforts to reduce amputation risk.
Copyright © 2013 Society for Vascular Surgery. Published by Mosby, Inc. All rights reserved.
Conflict of interest statement
Conflict of Interest Disclosures:
The authors report no conflicts of interest pertinent to this manuscript.
Figures




Comment in
-
Preventive measures for patients at risk for amputation from diabetes and peripheral arterial disease.Diabetes Care. 2014 Jun;37(6):e139-40. doi: 10.2337/dc14-0034. Diabetes Care. 2014. PMID: 24855171 Free PMC article. No abstract available.
References
-
- Newman AB, Sutton-Tyrrell K, Vogt MT, Kuller LH. Morbidity and mortality in hypertensive adults with a low ankle/arm blood pressure index.[see comment] JAMA. 1993;270:487–489. - PubMed
-
- O’Hare AM, Newman AB, Katz R, Fried LF, Stehman-Breen CO, Seliger SL, Siscovick DS, Shlipak MG. Cystatin c and incident peripheral arterial disease events in the elderly: Results from the cardiovascular health study. Archives of Internal Medicine. 2005;165:2666–2670. - PubMed
-
- Selvin E, Erlinger TP. Prevalence of and risk factors for peripheral arterial disease in the united states: Results from the natinoal health and nutrition examination survey, 1999–2000. Circulation. 2004;110:738–743. - PubMed
-
- McDermott MM. The magnitude of the problem of peripheral arterial disease: Epidemiology and clinical significance. Cleveland Clinic Journal of Medicine. 2006;73 (Suppl 4):S2–7. - PubMed
-
- Leng GC, Lee AJ, Fowkes FG, Whiteman M, Dunbar J, Housley E, Ruckley CV. Incidence, natural history and cardiovascular events in symptomatic and asymptomatic peripheral arterial disease in the general population. International Journal of Epidemiology. 1996;25:1172–1181. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
