

Prevalence of active convulsive epilepsy in sub-Saharan Africa and associated risk factors: cross-sectional and case-control studies
- PMID: 23375964
- PMCID: PMC3581814
- DOI: 10.1016/S1474-4422(13)70003-6
Prevalence of active convulsive epilepsy in sub-Saharan Africa and associated risk factors: cross-sectional and case-control studies
Abstract
Background: The prevalence of epilepsy in sub-Saharan Africa seems to be higher than in other parts of the world, but estimates vary substantially for unknown reasons. We assessed the prevalence and risk factors of active convulsive epilepsy across five centres in this region.
Methods: We did large population-based cross-sectional and case-control studies in five Health and Demographic Surveillance System centres: Kilifi, Kenya (Dec 3, 2007-July 31, 2008); Agincourt, South Africa (Aug 4, 2008-Feb 27, 2009); Iganga-Mayuge, Uganda (Feb 2, 2009-Oct 30, 2009); Ifakara, Tanzania (May 4, 2009-Dec 31, 2009); and Kintampo, Ghana (Aug 2, 2010-April 29, 2011). We used a three-stage screening process to identify people with active convulsive epilepsy. Prevalence was estimated as the ratio of confirmed cases to the population screened and was adjusted for sensitivity and attrition between stages. For each case, an age-matched control individual was randomly selected from the relevant centre's census database. Fieldworkers masked to the status of the person they were interviewing administered questionnaires to individuals with active convulsive epilepsy and control individuals to assess sociodemographic variables and historical risk factors (perinatal events, head injuries, and diet). Blood samples were taken from a randomly selected subgroup of 300 participants with epilepsy and 300 control individuals from each centre and were screened for antibodies to Toxocara canis, Toxoplasma gondii, Onchocerca volvulus, Plasmodium falciparum, Taenia solium, and HIV. We estimated odds ratios (ORs) with logistic regression, adjusted for age, sex, education, employment, and marital status.
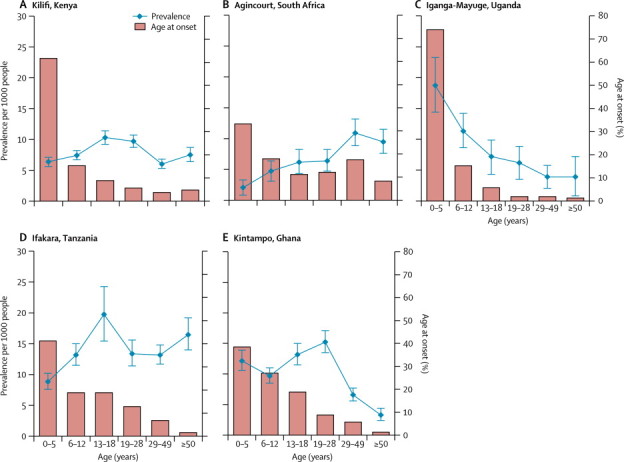
Results: 586,607 residents in the study areas were screened in stage one, of whom 1711 were diagnosed as having active convulsive epilepsy. Prevalence adjusted for attrition and sensitivity varied between sites: 7·8 per 1000 people (95% CI 7·5-8·2) in Kilifi, 7·0 (6·2-7·4) in Agincourt, 10·3 (9·5-11·1) in Iganga-Mayuge, 14·8 (13·8-15·4) in Ifakara, and 10·1 (9·5-10·7) in Kintampo. The 1711 individuals with the disorder and 2032 control individuals were given questionnaires. In children (aged <18 years), the greatest relative increases in prevalence were associated with difficulties feeding, crying, or breathing after birth (OR 10·23, 95% CI 5·85-17·88; p<0·0001); abnormal antenatal periods (2·15, 1·53-3·02; p<0·0001); and head injury (1·97, 1·28-3·03; p=0·002). In adults (aged ≥18 years), the disorder was significantly associated with admission to hospital with malaria or fever (2·28, 1·06-4·92; p=0·036), exposure to T canis (1·74, 1·27-2·40; p=0·0006), exposure to T gondii (1·39, 1·05-1·84; p=0·021), and exposure to O volvulus (2·23, 1·56-3·19; p<0·0001). Hypertension (2·13, 1·08-4·20; p=0·029) and exposure to T solium (7·03, 2·06-24·00; p=0·002) were risk factors for adult-onset disease.
Interpretation: The prevalence of active convulsive epilepsy varies in sub-Saharan Africa and that the variation is probably a result of differences in risk factors. Programmes to control parasitic diseases and interventions to improve antenatal and perinatal care could substantially reduce the prevalence of epilepsy in this region.
Copyright © 2013 Elsevier Ltd. All rights reserved.
Figures
Comment in
-
Epilepsy in Africa: caution and optimism.Lancet Neurol. 2013 Mar;12(3):220-2. doi: 10.1016/S1474-4422(12)70324-1. Epub 2013 Jan 31. Lancet Neurol. 2013. PMID: 23375963 No abstract available.
References
-
- Newton CR, Garcia H. Epilepsy in poor regions of the world. Lancet. 2012;380:1193–1201. - PubMed
-
- Preux P-M, Druet-Cabanc M. Epidemiology and aetiology of epilepsy in sub-Saharan Africa. Lancet Neurol. 2005;4:21–31. - PubMed
-
- Carter JA, Neville B, White S. Increased prevalence of epilepsy associated with severe falciparum malaria in children. Epilepsia. 2004;45:978–981. - PubMed
-
- Quet F, Guerchet M, Pion SD, Ngoungou EB, Nicoletti A, Preux PM. Meta-analysis of the association between cysticercosis and epilepsy in Africa. Epilepsia. 2009;51:830–837. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
