

Determination of the dynamics of healing at the tissue-implant interface by means of microcomputed tomography and functional apparent moduli
- PMID: 23377049
- PMCID: PMC4111564
- DOI: 10.11607/jomi.2614
Determination of the dynamics of healing at the tissue-implant interface by means of microcomputed tomography and functional apparent moduli
Abstract
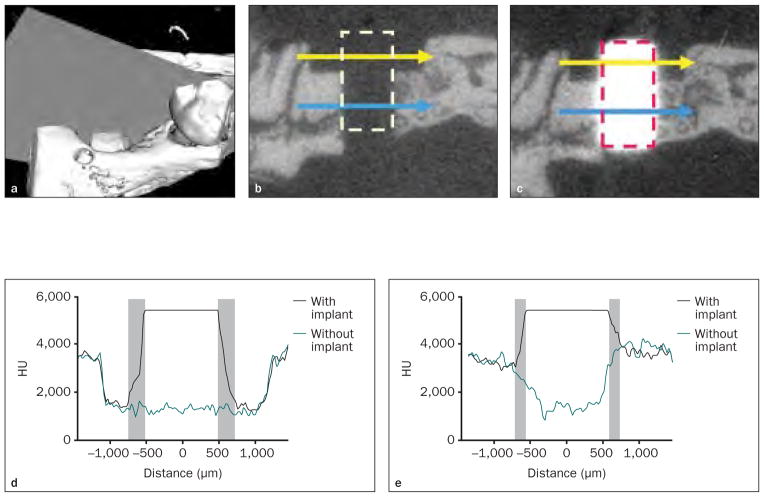
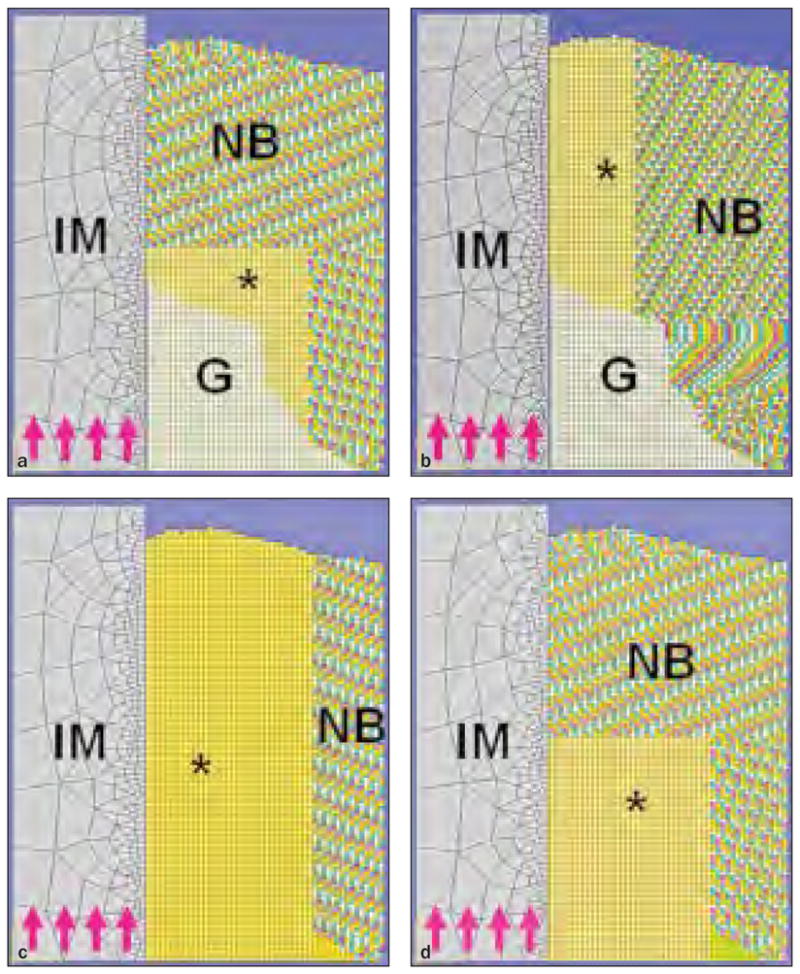
Purpose: It is currently a challenge to determine the biomechanical properties of the hard tissue-dental implant interface. Recent advances in intraoral imaging and tomographic methods, such as microcomputed tomography (micro-CT), provide three-dimensional details, offering significant potential to evaluate the bone-implant interface, but yield limited information regarding osseointegration because of physical scattering effects emanating from metallic implant surfaces. In the present study, it was hypothesized that functional apparent moduli (FAM), generated from functional incorporation of the peri-implant structure, would eliminate the radiographic artifact-affected layer and serve as a feasible means to evaluate the biomechanical dynamics of tissue-implant integration in vivo.
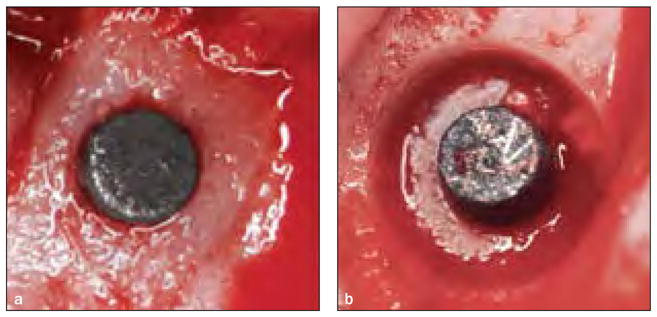
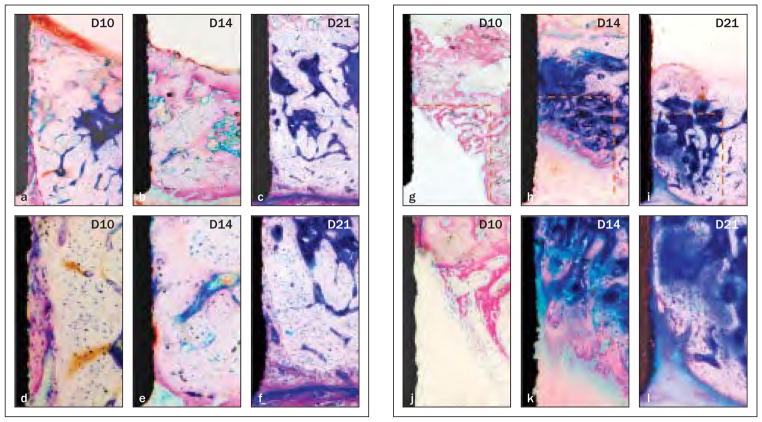
Materials and methods: Cylindric titanium mini-implants were placed in osteotomies and osteotomies with defects in rodent maxillae. The layers affected by radiographic artifacts were identified, and the pattern of tissue-implant integration was evaluated from histology and micro-CT images over a 21-day observation period. Analyses of structural information, FAM, and the relationship between FAM and interfacial stiffness (IS) were done before and after eliminating artifacts.
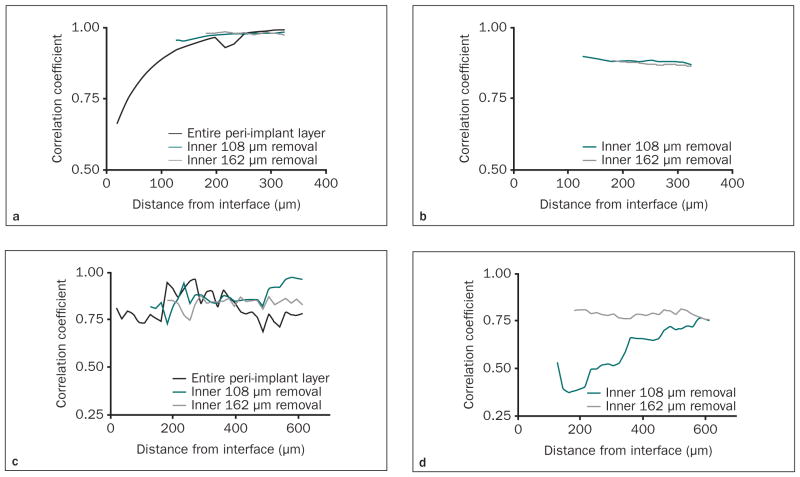
Results: Physical artifacts were present within a zone of about 100 to 150 Μm around the implant in both experimental defect situations (osteotomy alone and osteotomy + defect). All correlations were evaluated before and after eliminating the artifact-affected layers, most notably during the maturation period of osseointegration. A strong correlation existed between functional bone apparent modulus and IS within 300 Μm at the osteotomy defects (r > 0.9) and functional composite tissue apparent modulus in the osteotomy defects (r > 0.75).
Conclusion: Micro-CT imaging and FAM were of value in measuring the temporal process of tissue-implant integration in vivo. This approach will be useful to complement imaging technologies for longitudinal monitoring of osseointegration.
Conflict of interest statement
The authors reported no conflicts of interest related to this study.
Figures
References
-
- Franchi M, Fini M, Martini D, et al. Biological fixation of endosseous implants. Micron. 2005;36:665–671. - PubMed
-
- Turkyilmaz I, Sennerby L, McGlumphy EA, Tozum TF. Biomechanical aspects of primary implant stability: A human cadaver study. Clin Implant Dent Relat Res. 2009 Jun;11:113–119. - PubMed
-
- Qian L, Todo M, Matsushita Y, Koyano K. Effects of implant diameter, insertion depth, and loading angle on stress/strain fields in implant/jawbone systems: Finite element analysis. Int J Oral Maxillofac Implants. 2009;24:877–886. - PubMed
-
- Soballe K, Hansen ES, B-Rasmussen H, Jorgensen PH, Bunger C. Tissue ingrowth into titanium and hydroxyapatite-coated implants during stable and unstable mechanical conditions. J Orthop Res. 1992;10:285–299. - PubMed
-
- Albrektsson T, Linder L. A method for short- and long-term in vivo study of the bone-implant interface. Clin Orthop Relat Res. 1981;(159):269–273. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
