

Mild renal dysfunction and metabolites tied to low HDL cholesterol are associated with monocytosis and atherosclerosis
- PMID: 23378299
- PMCID: PMC4074592
- DOI: 10.1161/CIRCULATIONAHA.112.000682
Mild renal dysfunction and metabolites tied to low HDL cholesterol are associated with monocytosis and atherosclerosis
Abstract
Background: The number of circulating blood monocytes impacts atherosclerotic lesion size, and in mouse models, elevated levels of high-density lipoprotein cholesterol suppress blood monocyte counts and atherosclerosis. We hypothesized that individuals with mild renal dysfunction at increased cardiovascular risk would have reduced high-density lipoprotein levels, high blood monocyte counts, and accelerated atherosclerosis.
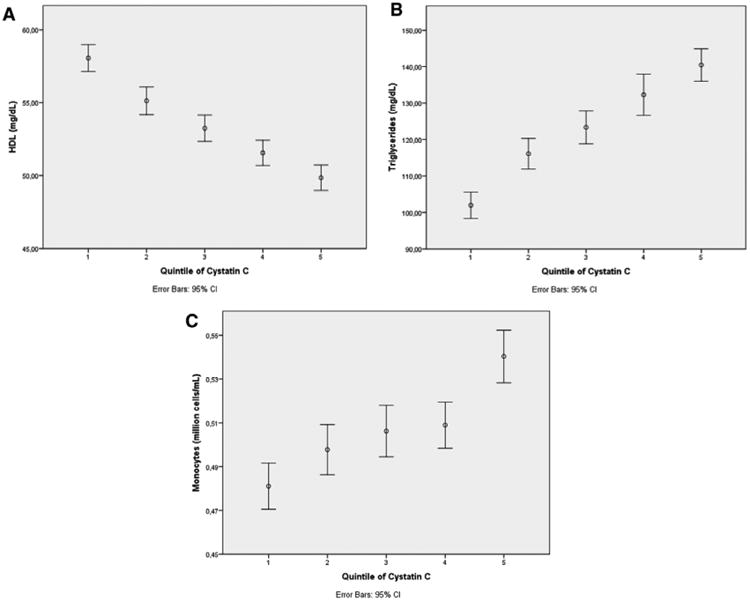
Methods and results: To test whether mild renal dysfunction is associated with an increase in a leukocyte subpopulation rich in monocytes that has a known association with future coronary events, we divided individuals from the Malmö Diet and Cancer study (MDC) into baseline cystatin C quintiles (n=4757). Lower levels of renal function were accompanied by higher monocyte counts, and monocytes were independently associated with carotid bulb intima-media thickness cross-sectionally (P=0.02). Cystatin C levels were positively and plasma high-density lipoprotein cholesterol levels negatively associated with monocyte counts at baseline, after adjustment for traditional risk factors. Several amino acid metabolites tied to low levels of high-density lipoprotein cholesterol and insulin resistance measured in a subset of individuals (n=752) by use of liquid chromatography-mass spectrometry were independently associated with a 22% to 34% increased risk of being in the top quartile of monocytes (P<0.05).
Conclusions: A low high-density lipoprotein cholesterol, insulin resistance phenotype occurs in subjects with mild renal dysfunction and is associated with elevated monocytes and atherosclerosis. High blood monocyte counts may represent a previously unrecognized mechanism underlying the strong relationship between cystatin C and cardiovascular risk.
Conflict of interest statement
Figures
Comment in
-
Cardiovascular disease: Monocytosis, atherosclerosis and increased cardiovascular risk in mild renal dysfunction.Nat Rev Nephrol. 2013 Apr;9(4):188. doi: 10.1038/nrneph.2013.32. Epub 2013 Feb 19. Nat Rev Nephrol. 2013. PMID: 23419348 No abstract available.
References
-
- Go AS, Chertow GM, Fan D, McCulloch CE, Hsu CY. Chronic kidney disease and the risks of death, cardiovascular events, and hospitalization. N Engl J Med. 2004;351:1296–1305. - PubMed
-
- Muntner P, He J, Astor BC, Folsom AR, Coresh J. Traditional and non-traditional risk factors predict coronary heart disease in chronic kidney disease: results from the Atherosclerosis Risk in Communities study. J Am Soc Nephrol. 2005;16:529–538. - PubMed
-
- Baigent C, Landray MJ, Reith C, Emberson J, Wheeler DC, Tomson C, Wanner C, Krane V, Cass A, Craig J, Neal B, Jiang L, Hooi LS, Levin A, Agodoa L, Gaziano M, Kasiske B, Walker R, Massy ZA, Feldt-Rasmussen B, Krairittichai U, Ophascharoensuk V, Fellström B, Holdaas H, Tesar V, Wiecek A, Grobbee D, de Zeeuw D, Grönhagen-Riska C, Dasgupta T, Lewis D, Herrington W, Mafham M, Majoni W, Wallendszus K, Grimm R, Pedersen T, Tobert J, Armitage J, Baxter A, Bray C, Chen Y, Chen Z, Hill M, Knott C, Parish S, Simpson D, Sleight P, Young A, Collins R SHARP Investigators. The effects of lowering LDL cholesterol with simvastatin plus ezetimibe in patients with chronic kidney disease (Study of Heart and Renal Protection): a randomised placebo-controlled trial. Lancet. 2011;377:2181–2192. - PMC - PubMed
-
- Wanner C, Krane V, März W, Olschewski M, Mann JF, Ruf G, Ritz E German Diabetes and Dialysis Study Investigators. Atorvastatin in patients with type 2 diabetes mellitus undergoing hemodialysis. N Engl J Med. 2005;353:238–248. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
