

Shrinking lung syndrome as a manifestation of pleuritis: a new model based on pulmonary physiological studies
- PMID: 23378468
- PMCID: PMC4112073
- DOI: 10.3899/jrheum.121048
Shrinking lung syndrome as a manifestation of pleuritis: a new model based on pulmonary physiological studies
Abstract
Objective: The pathophysiology of shrinking lung syndrome (SLS) is poorly understood. We sought to define the structural basis for this condition through the study of pulmonary mechanics in affected patients.
Methods: Since 2007, most patients evaluated for SLS at our institutions have undergone standardized respiratory testing including esophageal manometry. We analyzed these studies to define the physiological abnormalities driving respiratory restriction. Chest computed tomography data were post-processed to quantify lung volume and parenchymal density.
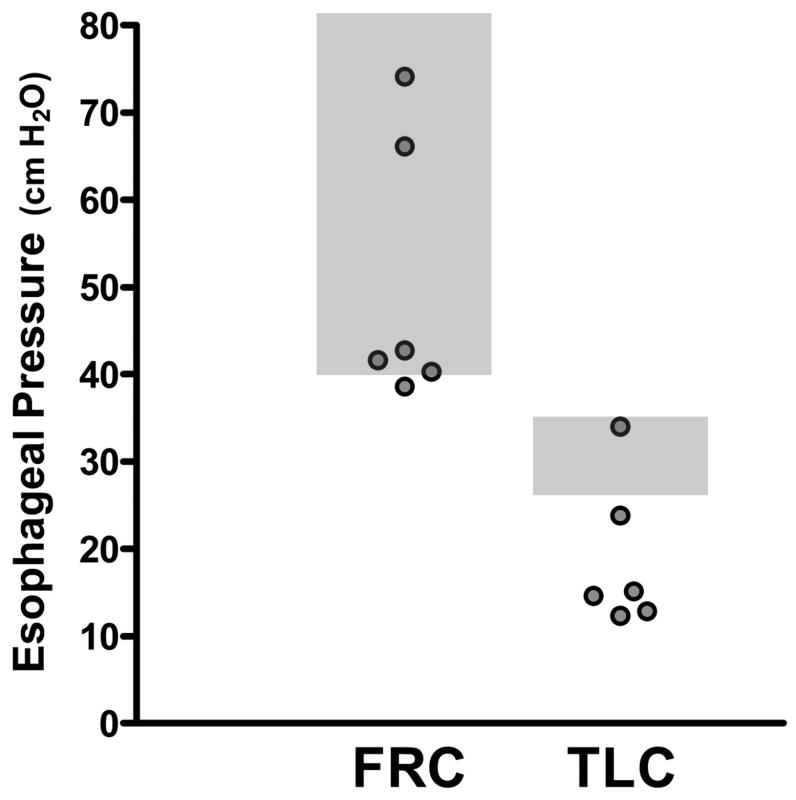
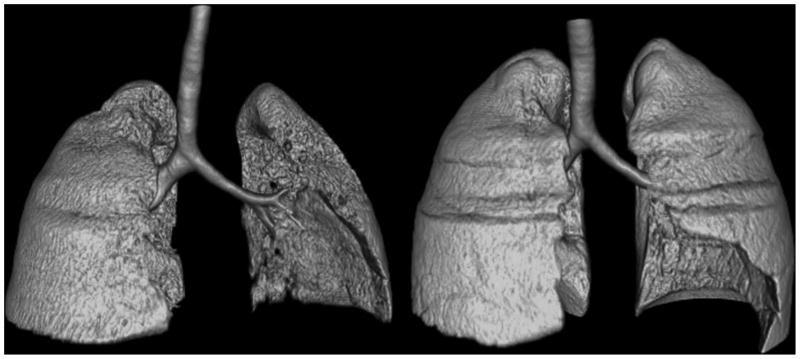
Results: Six cases met criteria for SLS. All presented with dyspnea as well as pleurisy and/or transient pleural effusions. Chest imaging results were free of parenchymal disease and corrected diffusing capacities were normal. Total lung capacities were 39%-50% of predicted. Maximal inspiratory pressures were impaired at high lung volumes, but not low lung volumes, in 5 patients. Lung compliance was strikingly reduced in all patients, accompanied by increased parenchymal density.
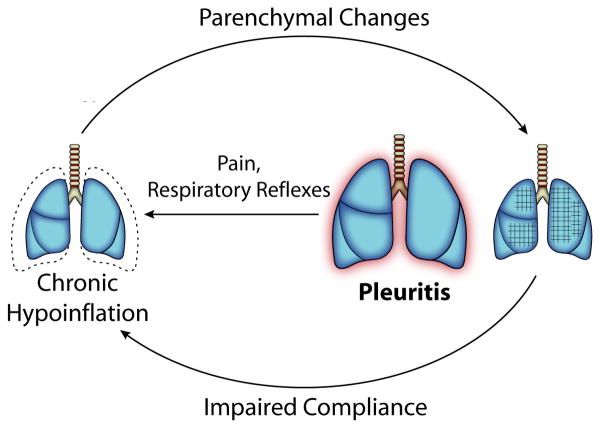
Conclusion: Patients with SLS exhibited symptomatic and/or radiographic pleuritis associated with 2 characteristic physiological abnormalities: (1) impaired respiratory force at high but not low lung volumes; and (2) markedly decreased pulmonary compliance in the absence of identifiable interstitial lung disease. These findings suggest a model in which pleural inflammation chronically impairs deep inspiration, for example through neural reflexes, leading to parenchymal reorganization that impairs lung compliance, a known complication of persistently low lung volumes. Together these processes could account for the association of SLS with pleuritis as well as the gradual symptomatic and functional progression that is a hallmark of this syndrome.
Figures
Comment in
-
Shrinking lung syndrome as a manifestation of pleuritis: are surface forces and surfactant the pathophysiological link?J Rheumatol. 2013 Nov;40(11):1926. doi: 10.3899/jrheum.130764. J Rheumatol. 2013. PMID: 24187160 No abstract available.
-
Dr. Henderson, et al reply.J Rheumatol. 2013 Nov;40(11):1926. doi: 10.3899/jrheum.130897. J Rheumatol. 2013. PMID: 24344358 No abstract available.
Similar articles
-
Shrinking lung syndrome as a presenting manifestation of systemic lupus erythematosus in a female Kuwaiti.Clin Rheumatol. 2006 May;25(3):412-4. doi: 10.1007/s10067-005-0020-5. Epub 2005 Dec 23. Clin Rheumatol. 2006. PMID: 16378163
-
Shrinking lung syndrome in systemic lupus erythematosus: a single-centre experience.Lupus. 2018 Mar;27(3):365-371. doi: 10.1177/0961203317722411. Epub 2017 Jul 31. Lupus. 2018. PMID: 28758573
-
Evaluating systemic lupus erythematosus patients for lung involvement.Lupus. 2012 Oct;21(12):1316-25. doi: 10.1177/0961203312454343. Epub 2012 Jul 19. Lupus. 2012. PMID: 22813546
-
Shrinking lung syndrome treated with rituximab in pediatric systemic lupus erythematosus: a case report and review of the literature.Pediatr Rheumatol Online J. 2021 Jan 6;19(1):7. doi: 10.1186/s12969-020-00491-0. Pediatr Rheumatol Online J. 2021. PMID: 33407629 Free PMC article. Review.
-
Presentation and prognosis of shrinking lung syndrome in systemic lupus erythematosus: report of four cases.Rheumatol Int. 2012 May;32(5):1391-6. doi: 10.1007/s00296-011-1863-5. Epub 2011 Mar 23. Rheumatol Int. 2012. PMID: 21431288 Review.
Cited by
-
Diaphragm Dysfunction: Diagnostic Approaches and Management Strategies.J Clin Med. 2016 Dec 5;5(12):113. doi: 10.3390/jcm5120113. J Clin Med. 2016. PMID: 27929389 Free PMC article. Review.
-
Rituximab effect in severe progressive connective tissue disease-related lung disease: preliminary data.Rheumatol Int. 2020 May;40(5):719-726. doi: 10.1007/s00296-020-04545-0. Epub 2020 Mar 10. Rheumatol Int. 2020. PMID: 32157369
-
Shrinking lung syndrome in autoimmune inflammatory diseases: A case series and review of literature.World J Emerg Med. 2022;13(3):254-256. doi: 10.5847/wjem.j.1920-8642.2022.041. World J Emerg Med. 2022. PMID: 35646220 Free PMC article. No abstract available.
-
Shrinking lung syndrome in systemic lupus erythematosus: A case series and review of the literature.Medicine (Baltimore). 2016 Aug;95(33):e4626. doi: 10.1097/MD.0000000000004626. Medicine (Baltimore). 2016. PMID: 27537601 Free PMC article. Review.
-
Lung Involvements in Rheumatic Diseases: Update on the Epidemiology, Pathogenesis, Clinical Features, and Treatment.Biomed Res Int. 2018 May 8;2018:6930297. doi: 10.1155/2018/6930297. eCollection 2018. Biomed Res Int. 2018. PMID: 29854780 Free PMC article. Review.
References
-
- Bertoli AM, Vilá LM, Apte M, Fessler BJ, Bastian HM, Reveille JD, et al. Systemic lupus erythematosus in multiethnic US cohort LUMINA XLVIII: factors predictive of pulmonary damage. Lupus. 2007;16:410–7. - PubMed
-
- Allen D, Fischer A, Bshouty Z, Robinson D, Peschken C, Hitchon C, et al. Evaluating systemic lupus erythematosus patients for lung involvement. Lupus. in press. - PubMed
-
- Ahmed S, Herrick A, O'Driscoll BR. Shrinking lung syndrome in patients without systemic lupus erythematosus. Arthritis Rheum. 2001;44:243–5. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous