

Pancreatic β-cell dysfunction and risk of new-onset diabetes after kidney transplantation
- PMID: 23378624
- PMCID: PMC3687295
- DOI: 10.2337/dc12-1894
Pancreatic β-cell dysfunction and risk of new-onset diabetes after kidney transplantation
Abstract
Objective: Chronic exposure to calcineurin inhibitors and corticosteroids poses renal transplant recipients (RTR) at high risk for development of new-onset diabetes after transplantation (NODAT). Pancreatic β-cell dysfunction may be crucial to the pathophysiology of NODAT and specific markers for β-cell dysfunction may have additive value for predicting NODAT in this population. Therefore, we prospectively investigated whether proinsulin, as a marker of pancreatic β-cell dysfunction, is associated with future development of NODAT and improves prediction of it.
Research design and methods: All RTR between 2001 and 2003 with a functioning graft for ≥1 year were considered eligible for inclusion, except for subjects with diabetes at baseline who were excluded. We recorded incidence of NODAT until April 2012.
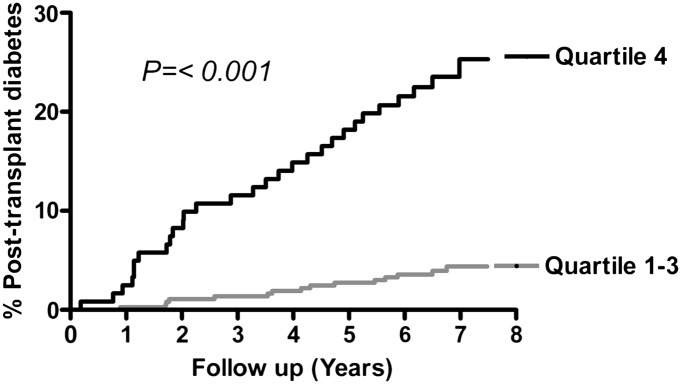
Results: A total of 487 RTR (age 50 ± 12 years, 55% men) participated at a median time of 6.0 (interquartile range [IQR], 2.6-11.5) years after transplantation. Median fasting proinsulin levels were 16.6 (IQR, 11.0-24.2) pmol/L. During median follow-up for 10.1 (IQR, 9.1-10.4) years, 42 (35%) RTR had development of NODAT in the highest quartile of the distribution of proinsulin versus 34 (9%) in the lowest three quartiles (P < 0.001). In Cox regression analyses, proinsulin (hazard ratio, 2.29; 95% CI, 1.85-2.83; P < 0.001) was strongly associated with NODAT development. This was independent of age, sex, calcineurine inhibitors, prednisolone use, components of the metabolic syndrome, or homeostasis model assessment.
Conclusions: In conclusion, fasting proinsulin is strongly associated with NODAT development in RTR. Our results highlight the role of β-cell dysfunction in the pathophysiology of NODAT and indicate the potential value of proinsulin for identification of RTR at increased risk for NODAT.
Figures
References
-
- Kuypers DR, Claes K, Bammens B, Evenepoel P, Vanrenterghem Y. Early clinical assessment of glucose metabolism in renal allograft recipients: diagnosis and prediction of post-transplant diabetes mellitus (PTDM). Nephrol Dial Transplant 2008;23:2033–2042 - PubMed
-
- Chadban S. New-onset diabetes after transplantation—should it be a factor in choosing an immunosuppressant regimen for kidney transplant recipients. Nephrol Dial Transplant 2008;23:1816–1818 - PubMed
-
- Kasiske BL, Snyder JJ, Gilbertson D, Matas AJ. Diabetes mellitus after kidney transplantation in the United States. Am J Transplant 2003;3:178–185 - PubMed
-
- Bee YM, Tan HC, Tay TL, Kee TY, Goh SY, Kek PC. Incidence and risk factors for development of new-onset diabetes after kidney transplantation. Ann Acad Med Singapore 2011;40:160–167 - PubMed
-
- Pfützner A, Pfützner AH, Larbig M, Forst T. Role of intact proinsulin in diagnosis and treatment of type 2 diabetes mellitus. Diabetes Technol Ther 2004;6:405–412 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
