

Glycation gap is associated with macroproteinuria but not with other complications in patients with type 2 diabetes
- PMID: 23378625
- PMCID: PMC3687281
- DOI: 10.2337/dc12-1780
Glycation gap is associated with macroproteinuria but not with other complications in patients with type 2 diabetes
Abstract
Objective: We investigated whether glycation gap (G-Gap), an index of intracellular glycation of proteins, was associated with diabetes complications.
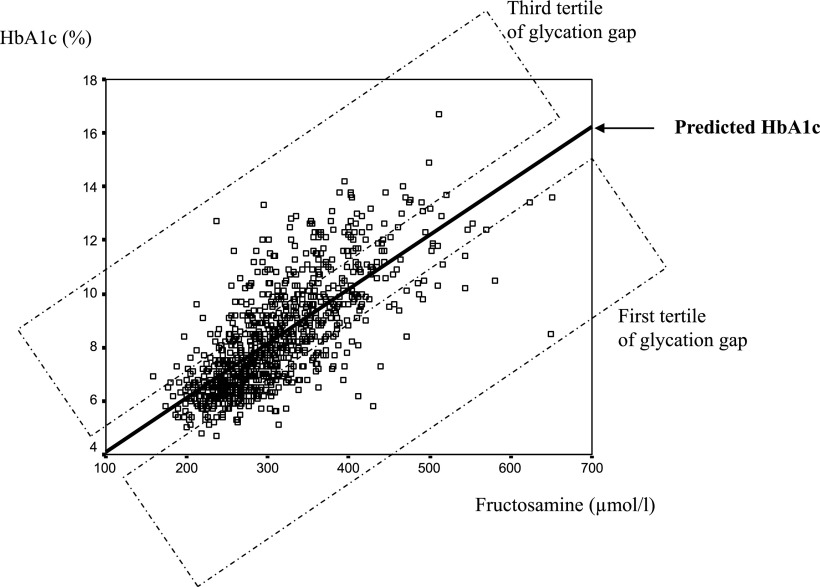
Research design and methods: We measured concomitantly HbA1c and fructosamine in 925 patients with type 2 diabetes to calculate the G-Gap, defined as the difference between measured HbA1c, and fructosamine-based predicted HbA1c. Patients were explored for retinopathy, nephropathy, peripheral neuropathy, cardiac autonomic neuropathy (n = 512), and silent myocardial ischemia (n = 506).
Results: Macroproteinuria was the only complication that was associated with G-Gap (prevalence in the first, second, and third tertile of G-Gap: 2.9, 6.2, and 11.0%, respectively; P < 0.001). The G-Gap was higher in patients with macroproteinuria than in those without (1.06 ± 1.62 vs. 0.03 ± 1.30%; P < 0.0001). Because HbA1c was associated with both G-Gap (HbA1c 7.0 ± 1.4, 7.9 ± 1.4, and 10.1 ± 1.8% in the first, second, and third G-Gap tertile, respectively; P < 0.0001) and macroproteinuria (HbA1c 8.8 ± 2.2% if macroproteinuria, 8.3 ± 2.0% if none; P < 0.05), and because it could have been a confounder, we matched 54 patients with macroproteinuria and 200 patients without for HbA1c. Because macroproteinuria was associated with lower serum albumin and fructosamine levels, which might account for higher G-Gap, we calculated in this subpopulation albumin-indexed fructosamine and G-Gap; macroproteinuria was independently associated with male sex (odds ratio [OR] 3.2 [95% CI 1.5-6.7]; P < 0.01), hypertension (2.9 [1.1-7.5]; P < 0.05), and the third tertile of albumin-indexed G-Gap (2.3 [1.1-4.4]; P < 0.05) in multivariate analysis.
Conclusions: In type 2 diabetic patients, G-Gap was associated with macroproteinuria, independently of HbA1c, albumin levels, and confounding factors, suggesting a specific role of intracellular glycation susceptibility on kidney glomerular changes.
Figures
References
-
- Rohlfing CL, Wiedmeyer HM, Little RR, England JD, Tennill A, Goldstein DE. Defining the relationship between plasma glucose and HbA(1c): analysis of glucose profiles and HbA(1c) in the Diabetes Control and Complications Trial. Diabetes Care 2002;25:275–278 - PubMed
-
- Hempe JM, Gomez R, McCarter RJ, Jr, Chalew SA. High and low hemoglobin glycation phenotypes in type 1 diabetes: a challenge for interpretation of glycemic control. J Diabetes Complications 2002;16:313–320 - PubMed
-
- Cohen RM, Holmes YR, Chenier TC, Joiner CH. Discordance between HbA1c and fructosamine: evidence for a glycosylation gap and its relation to diabetic nephropathy. Diabetes Care 2003;26:163–167 - PubMed
-
- Rodríguez-Segade S, Rodríguez J, Cabezas-Agricola JM, Casanueva FF, Camiña F. Progression of nephropathy in type 2 diabetes: the glycation gap is a significant predictor after adjustment for glycohemoglobin (Hb A1c). Clin Chem 2011;57:264–271 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
