

Factors associated with peritoneal metastasis in non-serosa-invasive gastric cancer: a retrospective study of a prospectively-collected database
- PMID: 23379700
- PMCID: PMC3641004
- DOI: 10.1186/1471-2407-13-57
Factors associated with peritoneal metastasis in non-serosa-invasive gastric cancer: a retrospective study of a prospectively-collected database
Abstract
Background: Peritoneal dissemination is the most common type of recurrence in advanced gastric cancer. The main mechanism is thought to be via the exfoliation of free cancer cells (FCCs) from tumor in the gastric serosa. The frequency of recurrence thus increases once the tumor cells penetrate the serosa. However, this type of recurrence also occurs in patients without serosal invasion, though the mechanisms responsible for have not been fully established. We therefore investigated the factors associated with peritoneal dissemination in patients with non-serosa-invasive gastric cancer.
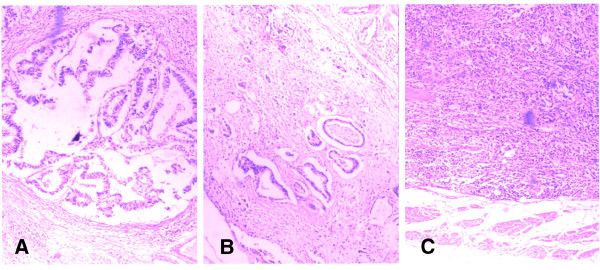
Methods: A total of 685 patients with non-serosa-invasive gastric cancer who underwent curative resection with retrieval of more than 15 nodes were selected. The associations between clinicopathological features and peritoneal dissemination were analyzed. Among them, the tumor infiltrating growth pattern (INF) were classified into α, β and γ according to the Japanese Classification of Gastric Carcinoma (JCGC).
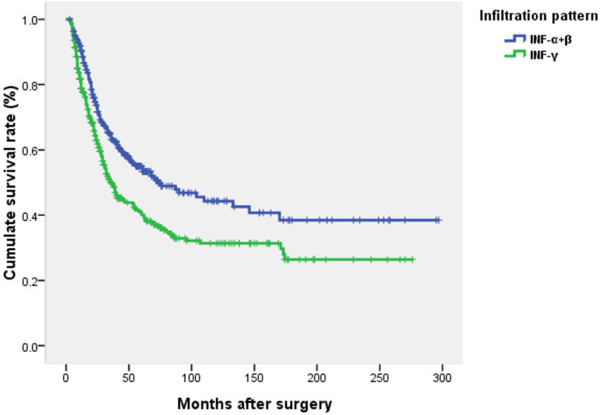
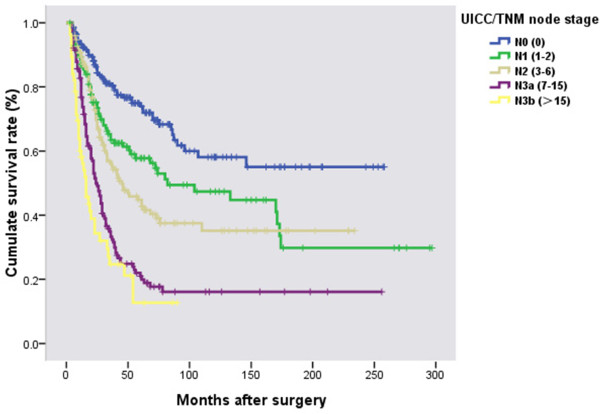
Results: The overall incidence of peritoneal metastasis was 20% (137/685). Age, Borrmann type, differentiation, INF, nodal status and free cancer cells (FCCs) were correlated with peritoneal dissemination using univariate analysis. However, only INF, Borrmann type and TNM node stage were identified as independent correlated factors with peritoneal metastasis by multivariate analysis when FCCs were excluded, and these were also prognostic factors. Peritoneal dissemination was more common in patients with INFγ, Borrmann III/IV and N3 stage. Among patients without FCCs, nodal involvement or vessel invasion, only INF remained an independent associated factor according to multivariate analysis.
Conclusions: Tumor infiltrating growth pattern (INF), together with Borrmann type and TNM node stage, are important factors associated with peritoneal metastasis in non-serosa-invasive gastric cancer.
Figures

References
-
- Leung WK, Wu MS, Kakugawa Y, Kim JJ, Yeoh KG, Goh KL, Wu KC, Wu DC, Sollano J, Kachintorn U, Gotoda T, Lin JT, You WC, Ng EK, Sung JJ. Asia Pacific Working Group on Gastric Cancer. Screening for gastric cancer in Asia: current evidence and practice. Lancet Oncol. 2008;9(3):279–287. doi: 10.1016/S1470-2045(08)70072-X. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
