

Closing the personalized medicine information gap: HER2 test documentation practice
- PMID: 23379747
- PMCID: PMC3919466
Closing the personalized medicine information gap: HER2 test documentation practice
Abstract
Background: Uncertainty about human epidermal growth factor receptor-2 (HER2) testing practice in Canada continues to hinder efforts to improve personalized medicine. Pathologists routinely perform HER2 assessment for all tumors > 1 cm, and pathology is reported centrally to the provincial cancer registry.
Objectives: To understand patterns of HER2 test documentation for early-stage breast cancer (BC) patients in Ontario's centralized pathology reporting system.
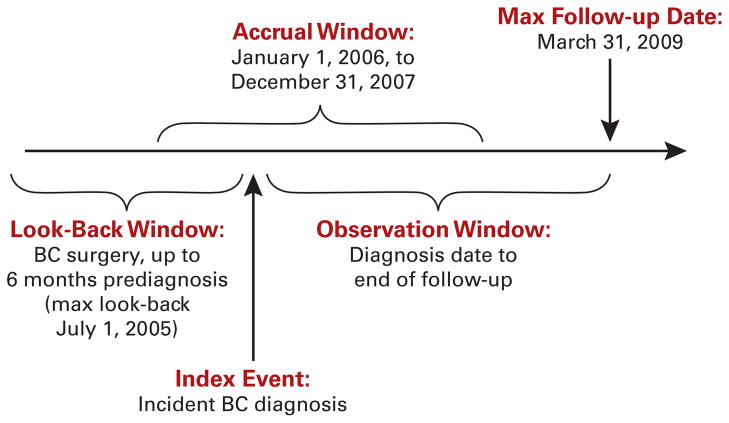
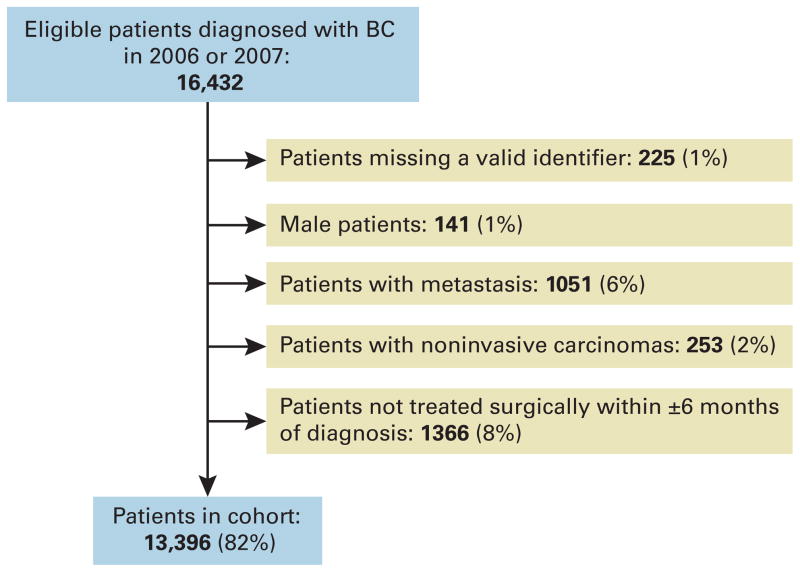
Study design: Retrospective cohort study of central HER2 test documentation in early-stage BC patients diagnosed in 2006-2007.
Methods: Cohort and staging information was derived from cancer registry and admissions data. Linkage across administrative databases provided data on surgical and radiologic treatment, sociodemographic factors, diagnosis setting, and comorbidities. Pathology reports from the provincial cancer registry were reviewed for HER2 testing, hormone receptor, and grade. Unadjusted and adjusted odds ratios were calculated to determine factors related to HER2 documentation.
Results: A HER2 test was documented for 66% of 13,396 patients. HER2 documentation was associated with stage, hormone receptor, and tumor grade documentation. Higher stage and grade at diagnosis were also associated with HER2 documentation. All models suggested variable regional documentation patterns. Documentation did not differ by sociodemographic factors, presence of comorbidities, or surgical procedure.
Conclusions: Despite a universal testing policy, the rate of centralized HER2 test documentation was lower than expected and related to disease severity. Differences in regional reporting likely reflect ascertainment bias inherent to centralized pathology reporting rather than testing access. Improved HER2 reporting is encouraged for cancer registration, quality-of-care measurement, and program evaluation.
Figures
Similar articles
-
HER2 evaluation and its impact on breast cancer treatment decisions.Public Health Genomics. 2012;15(1):1-10. doi: 10.1159/000325746. Epub 2011 May 3. Public Health Genomics. 2012. PMID: 21540562 Free PMC article.
-
Adherence to human epidermal growth factor receptor-2 testing and adjuvant trastuzumab treatment guidelines in Ontario.J Oncol Pharm Pract. 2020 Mar;26(2):379-385. doi: 10.1177/1078155219850299. Epub 2019 Jun 2. J Oncol Pharm Pract. 2020. PMID: 31156051
-
ReCAP: Treatment Patterns and Cost of Care Associated With Initial Therapy Among Patients Diagnosed With Operable Early-Stage Human Epidermal Growth Factor Receptor 2-Overexpressed Breast Cancer in the United States: A Real-World Retrospective Study.J Oncol Pract. 2016 Feb;12(2):159-67. doi: 10.1200/JOP.2015.004747. Epub 2015 Sep 22. J Oncol Pract. 2016. PMID: 26395563
-
Current status of HER2 testing.Oncology. 2002;63 Suppl 1:25-32. doi: 10.1159/000066204. Oncology. 2002. PMID: 12422052 Review.
-
HER2 testing in breast cancer: NCCN Task Force report and recommendations.J Natl Compr Canc Netw. 2006 Jul;4 Suppl 3:S1-22; quiz S23-4. J Natl Compr Canc Netw. 2006. PMID: 16813731 Review.
Cited by
-
Recommendations for human epidermal growth factor receptor 2 testing in breast cancer: American Society of Clinical Oncology/College of American Pathologists clinical practice guideline update.Arch Pathol Lab Med. 2014 Feb;138(2):241-56. doi: 10.5858/arpa.2013-0953-SA. Epub 2013 Oct 7. Arch Pathol Lab Med. 2014. PMID: 24099077 Free PMC article.
-
Breast cancer multigene testing trends and impact on chemotherapy use.Am J Manag Care. 2016 May 1;22(5):e153-60. Am J Manag Care. 2016. PMID: 27266581 Free PMC article.
-
Are there socio-economic inequalities in utilization of predictive biomarker tests and biological and precision therapies for cancer? A systematic review and meta-analysis.BMC Med. 2020 Oct 23;18(1):282. doi: 10.1186/s12916-020-01753-0. BMC Med. 2020. PMID: 33092592 Free PMC article.
References
-
- Canadian Cancer Society’s Steering Committee on Cancer Statistics. Canadian Cancer Statistics 2011. Toronto, Canada: Canadian Cancer Society; 2011.
-
- Slamon DJ, Clark GM, Wong SG, Levin WJ, Ullrich A, McGuire WL. Human breast cancer: correlation of relapse and survival with amplification of the HER-2/neu oncogene. Science. 1987;235(4785):177–182. - PubMed
-
- Slamon DJ, Godolphin W, Jones LA, et al. Studies of the HER-2/neu proto-oncogene in human breast and ovarian cancer. Science. 1989;244(4905):707–712. - PubMed
-
- Dahabreh IJ, Linardou H, Siannis F, Fountzilas G, Murray S. Trastuzumab in the adjuvant treatment of early-stage breast cancer: a systematic review and meta-analysis of randomized controlled trials. Oncologist. 2008;13(6):620–630. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
