

Impact of pretransplantation conditioning regimens on outcomes of allogeneic transplantation for chemotherapy-unresponsive diffuse large B cell lymphoma and grade III follicular lymphoma
- PMID: 23380340
- PMCID: PMC3650915
- DOI: 10.1016/j.bbmt.2013.01.024
Impact of pretransplantation conditioning regimens on outcomes of allogeneic transplantation for chemotherapy-unresponsive diffuse large B cell lymphoma and grade III follicular lymphoma
Abstract
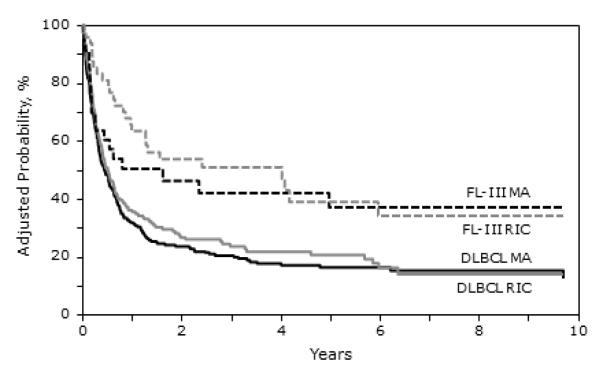
Patients with chemorefractory non-Hodgkin lymphomas generally have a poor prognosis. We used the observational database of the Center for International Blood and Marrow Transplant Research to study the outcome of 533 patients with refractory diffuse large B cell lymphoma (DLBCL) or grade III follicular lymphoma (FL-III) who underwent allogeneic hematopoietic cell transplantation (allo-HCT) using either myeloablative (MA; n = 307) or reduced-intensity/nonmyeloablative conditioning (RIC/NST; n = 226) between 1998 and 2010. We analyzed nonrelapse mortality (NRM), relapse/progression, progression-free survival (PFS), and overall survival (OS). Only 45% of the patients at transplantation had a Karnofsky performance score of ≥90%. Median follow-up of surviving patients after MA and RIC/NST allo-HCT is 35 months and 30 months, respectively. At 3 years, MA allo-HCT was associated with a higher NRM compared with RIC/NST (53% versus 42%; P = .03), similar PFS (19% versus 23%; P = .40), and lower OS (19% versus 28%; P = .02), respectively. On multivariate analysis, FL-III histology was associated with lower NRM (relative risk [RR], .52), reduced risk of relapse/progression (RR, .42), and superior PFS (RR, .51) and OS (RR, .53), whereas MA conditioning was associated with reduced risk of relapse/progression (RR, .66). Despite a refractory state, a small subset of DLBCL and FL-III patients can attain durable remissions after allo-HCT. Conditioning regimen intensity was not associated with PFS and OS despite a higher risk of relapse/progression with RIC/NST allo-HCT.
Copyright © 2013 American Society for Blood and Marrow Transplantation. Published by Elsevier Inc. All rights reserved.
Figures

References
-
- Philip T, Armitage JO, Spitzer G, et al. High-dose therapy and autologous bone marrow transplantation after failure of conventional chemotherapy in adults with intermediate-grade or high-grade non-Hodgkin’s lymphoma. N.Engl.J.Med. 1987;316:1493–1498. - PubMed
-
- Philip T, Guglielmi C, Hagenbeek A, et al. Autologous bone marrow transplantation as compared with salvage chemotherapy in relapses of chemotherapy-sensitive non-Hodgkin’s lymphoma. N.Engl.J.Med. 1995;333:1540–1545. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
