

Dietary and supplemental calcium intake and cardiovascular disease mortality: the National Institutes of Health-AARP diet and health study
- PMID: 23381719
- PMCID: PMC3756477
- DOI: 10.1001/jamainternmed.2013.3283
Dietary and supplemental calcium intake and cardiovascular disease mortality: the National Institutes of Health-AARP diet and health study
Abstract
Importance: Calcium intake has been promoted because of its proposed benefit on bone health, particularly among the older population. However, concerns have been raised about the potential adverse effect of high calcium intake on cardiovascular health.
Objective: To investigate whether intake of dietary and supplemental calcium is associated with mortality from total cardiovascular disease (CVD), heart disease, and cerebrovascular diseases.
Design and setting: Prospective study from 1995 through 1996 in California, Florida, Louisiana, New Jersey, North Carolina, and Pennsylvania and the 2 metropolitan areas of Atlanta, Georgia, and Detroit, Michigan.
Participants: A total of 388 229 men and women aged 50 to 71 years from the National Institutes of Health-AARP Diet and Health Study.
Main outcome measures: Dietary and supplemental calcium intake was assessed at baseline (1995-1996). Supplemental calcium intake included calcium from multivitamins and individual calcium supplements. Cardiovascular disease deaths were ascertained using the National Death Index. Multivariate Cox proportional hazards regression models adjusted for demographic, lifestyle, and dietary variables were used to estimate relative risks (RRs) and 95% CIs.
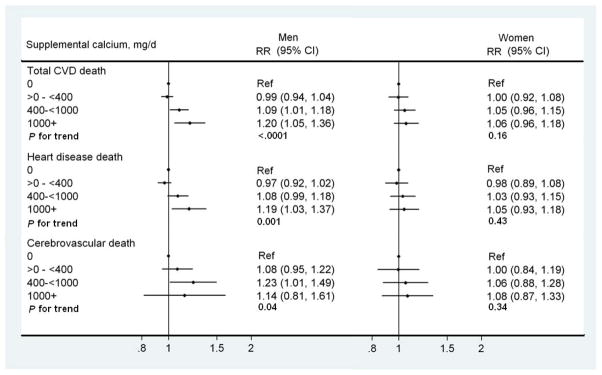
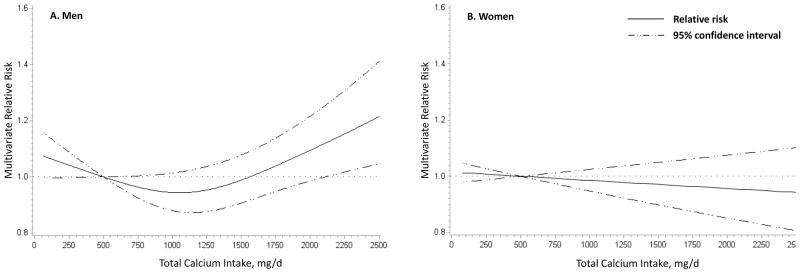
Results: During a mean of 12 years of follow-up, 7904 and 3874 CVD deaths in men and women, respectively, were identified. Supplements containing calcium were used by 51% of men and 70% of women. In men, supplemental calcium intake was associated with an elevated risk of CVD death (RR>1000 vs 0 mg/d, 1.20; 95% CI, 1.05-1.36), more specifically with heart disease death (RR, 1.19; 95% CI, 1.03-1.37) but not significantly with cerebrovascular disease death (RR, 1.14; 95% CI, 0.81-1.61). In women, supplemental calcium intake was not associated with CVD death (RR, 1.06; 95% CI, 0.96-1.18), heart disease death (1.05; 0.93-1.18), or cerebrovascular disease death (1.08; 0.87-1.33). Dietary calcium intake was unrelated to CVD death in either men or women.
Conclusions and relevance: Our findings suggest that high intake of supplemental calcium is associated with an excess risk of CVD death in men but not in women. Additional studies are needed to investigate the effect of supplemental calcium use beyond bone health.
Figures
Comment in
-
Are calcium supplements harmful to cardiovascular disease?JAMA Intern Med. 2013 Apr 22;173(8):647-8. doi: 10.1001/jamainternmed.2013.3769. JAMA Intern Med. 2013. PMID: 23380757 No abstract available.
-
Risk factors: High calcium intake linked to cardiac death.Nat Rev Cardiol. 2013 Apr;10(4):181. doi: 10.1038/nrcardio.2013.22. Epub 2013 Feb 26. Nat Rev Cardiol. 2013. PMID: 23438688 No abstract available.
-
[Does calcium intake affect cardiovascular mortality?--Intake of supplemental calcium holds risks--especially for men].Dtsch Med Wochenschr. 2013 Jul;138(28-29):1448. doi: 10.1055/s-0032-1329053. Epub 2013 Jul 2. Dtsch Med Wochenschr. 2013. PMID: 23821445 German. No abstract available.
-
Calcium supplements associated with increased risk of cardiovascular death in men but not women.Evid Based Nurs. 2014 Jul;17(3):90. doi: 10.1136/eb-2013-101460. Epub 2013 Aug 29. Evid Based Nurs. 2014. PMID: 23990583 No abstract available.
-
Dietary and supplemental calcium intake and mortality.JAMA Intern Med. 2013 Oct 28;173(19):1840. doi: 10.1001/jamainternmed.2013.9267. JAMA Intern Med. 2013. PMID: 24165840 No abstract available.
-
Dietary and supplemental calcium intake and mortality.JAMA Intern Med. 2013 Oct 28;173(19):1840-1. doi: 10.1001/jamainternmed.2013.9276. JAMA Intern Med. 2013. PMID: 24165841 No abstract available.
-
Dietary and supplemental calcium intake and mortality.JAMA Intern Med. 2013 Oct 28;173(19):1841. doi: 10.1001/jamainternmed.2013.9260. JAMA Intern Med. 2013. PMID: 24165842 No abstract available.
-
Dietary and supplemental calcium intake and mortality--reply.JAMA Intern Med. 2013 Oct 28;173(19):1841-2. doi: 10.1001/jamainternmed.2013.9232. JAMA Intern Med. 2013. PMID: 24165843 No abstract available.
References
-
- Hennekens CH, Barice EJ. Calcium supplements and risk of myocardial infarction: a hypothesis formulated but not yet adequately tested. Am J Med. 2011;124(12):1097–8. - PubMed
-
- Reid IR, Bolland MJ, Grey A. Calcium supplements and risk of myocardial infarction: an hypothesis twice tested. Am J Med. 2012;125(4):e15. author reply e17. - PubMed
-
- Bucher HC, Cook RJ, Guyatt GH, et al. Effects of dietary calcium supplementation on blood pressure. A meta-analysis of randomized controlled trials. JAMA. 1996;275(13):1016–22. - PubMed
-
- Cappuccio FP, Elliott P, Allender PS, Pryer J, Follman DA, Cutler JA. Epidemiologic association between dietary calcium intake and blood pressure: a meta-analysis of published data. Am J Epidemiol. 1995;142(9):935–45. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
