

Nonalcoholic fatty liver disease: MR imaging of liver proton density fat fraction to assess hepatic steatosis
- PMID: 23382291
- PMCID: PMC3632805
- DOI: 10.1148/radiol.12120896
Nonalcoholic fatty liver disease: MR imaging of liver proton density fat fraction to assess hepatic steatosis
Abstract
Purpose: To evaluate the diagnostic performance of magnetic resonance (MR) imaging-estimated proton density fat fraction (PDFF) for assessing hepatic steatosis in nonalcoholic fatty liver disease (NAFLD) by using centrally scored histopathologic validation as the reference standard.
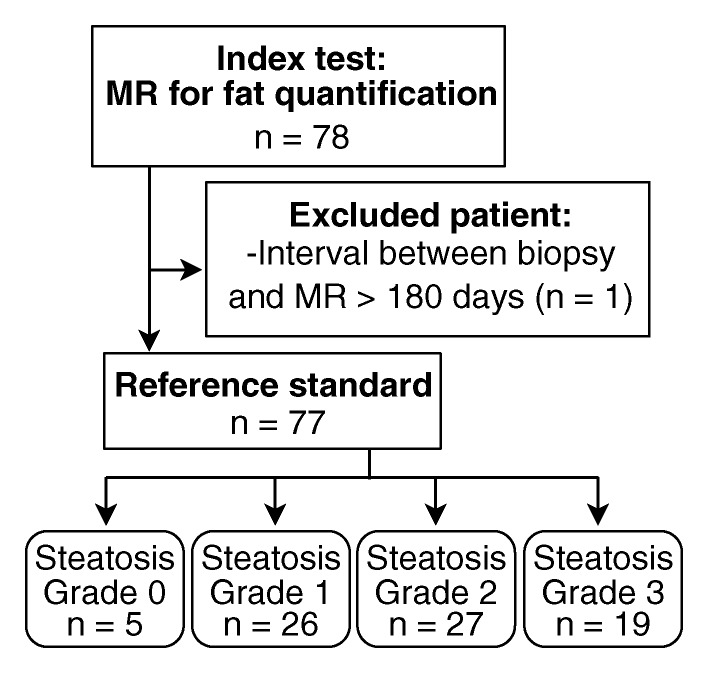
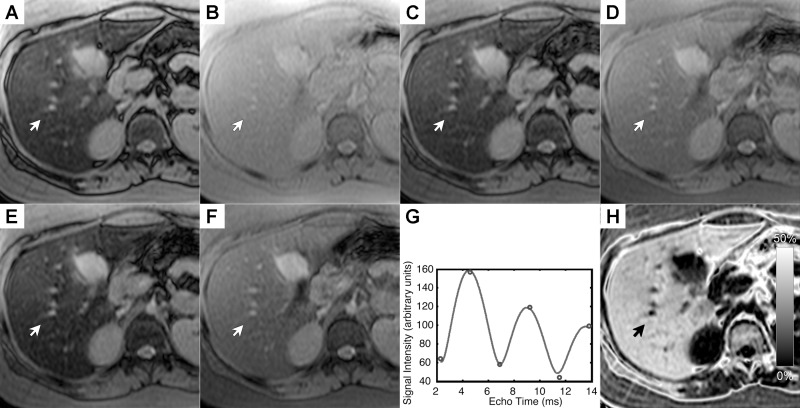
Materials and methods: This prospectively designed, cross-sectional, internal review board-approved, HIPAA-compliant study was conducted in 77 patients who had NAFLD and liver biopsy. MR imaging-PDFF was estimated from magnitude-based low flip angle multiecho gradient-recalled echo images after T2* correction and multifrequency fat modeling. Histopathologic scoring was obtained by consensus of the Nonalcoholic Steatohepatitis (NASH) Clinical Research Network Pathology Committee. Spearman correlation, additivity and variance stabilization for regression for exploring the effect of a number of potential confounders, and receiver operating characteristic analyses were performed.
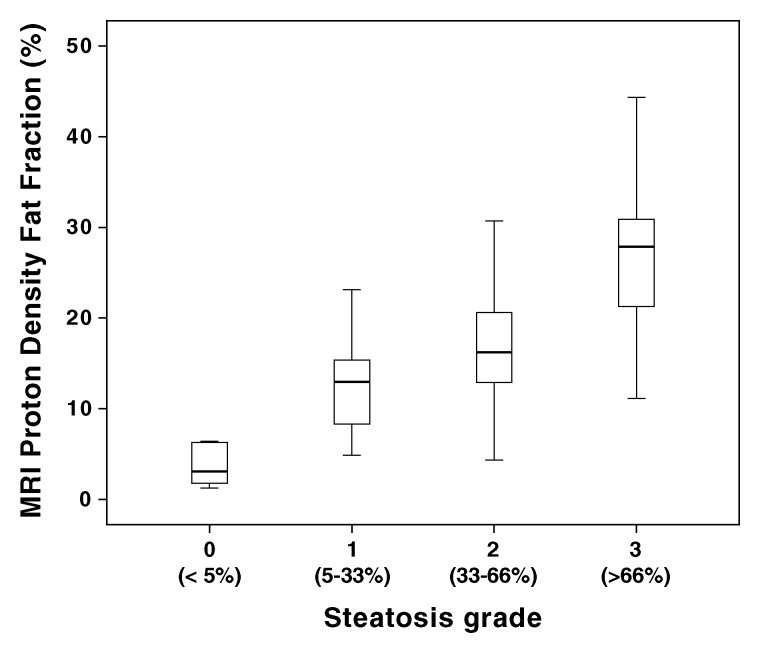
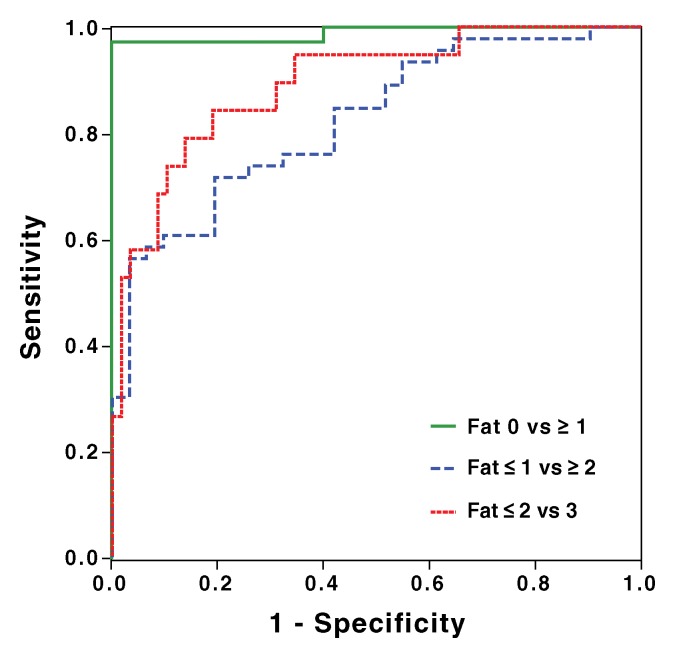
Results: Liver MR imaging-PDFF was systematically higher, with higher histologic steatosis grade (P < .001), and was significantly correlated with histologic steatosis grade (ρ = 0.69, P < .001). The correlation was not confounded by age, sex, lobular inflammation, hepatocellular ballooning, NASH diagnosis, fibrosis, or magnetic field strength (P = .65). Area under the receiver operating characteristic curves was 0.989 (95% confidence interval: 0.968, 1.000) for distinguishing patients with steatosis grade 0 (n = 5) from those with grade 1 or higher (n = 72), 0.825 (95% confidence interval: 0.734, 0.915) to distinguish those with grade 1 or lower (n = 31) from those with grade 2 or higher (n = 46), and 0.893 (95% confidence interval: 0.809, 0.977) to distinguish those with grade 2 or lower (n = 58) from those with grade 3 (n = 19).
Conclusion: MR imaging-PDFF showed promise for assessment of hepatic steatosis grade in patients with NAFLD. For validation, further studies with larger sample sizes are needed.
© RSNA, 2013.
Figures
References
-
- Bellentani S, Scaglioni F, Marino M, Bedogni G. Epidemiology of non-alcoholic fatty liver disease. Dig Dis 2010;28(1):155–161 - PubMed
-
- Schwimmer JB, Deutsch R, Kahen T, Lavine JE, Stanley C, Behling C. Prevalence of fatty liver in children and adolescents. Pediatrics 2006;118(4):1388–1393 - PubMed
-
- Angulo P, Lindor KD. Non-alcoholic fatty liver disease. J Gastroenterol Hepatol 2002;17(Suppl):S186–S190 - PubMed
-
- Jou J, Choi SS, Diehl AM. Mechanisms of disease progression in nonalcoholic fatty liver disease. Semin Liver Dis 2008;28(4):370–379 - PubMed
-
- Pais R, Pascale A, Fedchuck L, Charlotte F, Poynard T, Ratziu V. Progression from isolated steatosis to steatohepatitis and fibrosis in nonalcoholic fatty liver disease. Clin Res Hepatol Gastroenterol 2011;35(1):23–28 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
