

MRSA transmission on a neonatal intensive care unit: epidemiological and genome-based phylogenetic analyses
- PMID: 23382995
- PMCID: PMC3561456
- DOI: 10.1371/journal.pone.0054898
MRSA transmission on a neonatal intensive care unit: epidemiological and genome-based phylogenetic analyses
Abstract
Background: Methicillin-resistant Staphylococcus aureus (MRSA) may cause prolonged outbreaks of infections in neonatal intensive care units (NICUs). While the specific factors favouring MRSA spread on neonatal wards are not well understood, colonized infants, their relatives, or health-care workers may all be sources for MRSA transmission. Whole-genome sequencing may provide a new tool for elucidating transmission pathways of MRSA at a local scale.
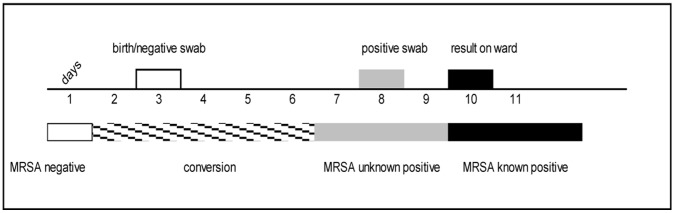
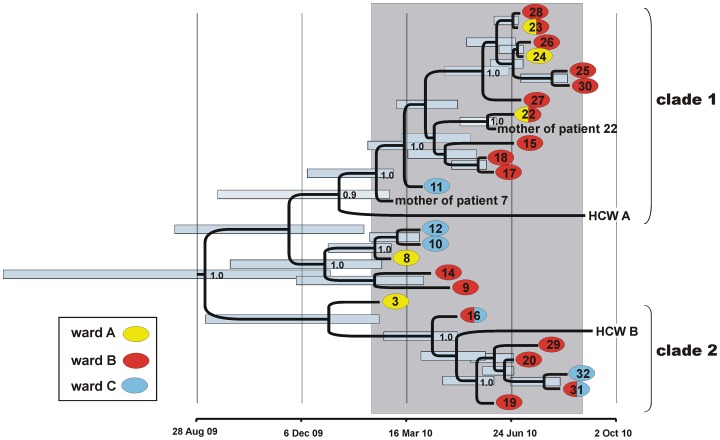
Methods and findings: We applied whole-genome sequencing to trace MRSA spread in a NICU and performed a case-control study to identify risk factors for MRSA transmission. MRSA genomes had accumulated sequence variation sufficiently fast to reflect epidemiological linkage among individual patients, between infants and their mothers, and between infants and staff members, such that the relevance of individual nurses' nasal MRSA colonization for prolonged transmission could be evaluated. In addition to confirming previously reported risk factors, we identified an increased risk of transmission from infants with as yet unknown MRSA colonisation, in contrast to known MRSA-positive infants.
Conclusions: The integration of epidemiological (temporal, spatial) and genomic data enabled the phylogenetic testing of several hypotheses on specific MRSA transmission routes within a neonatal intensive-care unit. The pronounced risk of transmission emanating from undetected MRSA carriers suggested that increasing the frequency or speed of microbiological diagnostics could help to reduce transmission of MRSA.
Conflict of interest statement
Figures
References
-
- Khoury J, Jones M, Grim A, Dunne WM Jr, Fraser V (2005) Eradication of methicillin-resistant Staphylococcus aureus from a neonatal intensive care unit by active surveillance and aggressive infection control measures. Infect Control Hosp Epidemiol 26: 616–621. - PubMed
-
- Andersen BM, Lindemann R, Bergh K, Nesheim BI, Syversen G, et al. (2002) Spread of methicillin-resistant Staphylococcus aureus in a neonatal intensive unit associated with understaffing, overcrowding and mixing of patients. J Hosp Infect 50: 18–24. - PubMed
-
- Gould IM, Girvan EK, Browning RA, MacKenzie FM, Edwards GF (2009) Report of a hospital neonatal unit outbreak of community-associated methicillin-resistant Staphylococcus aureus . Epidemiol Infect 137: 1242–1248. - PubMed
-
- McAdams RM, Ellis MW, Trevino S, Rajnik M (2008) Spread of methicillin-resistant Staphylococcus aureus USA300 in a neonatal intensive care unit. Pediatr Int 50: 810–815. - PubMed
-
- Vergnano S, Menson E, Smith Z, Kennea N, Embleton N, et al. (2011) Characteristics of invasive Staphylococcus aureus in United Kingdom neonatal units. Pediatr Infect Dis J 30: 850–854. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
