

The impact of syphilis screening among female sex workers in China: a modelling study
- PMID: 23383249
- PMCID: PMC3559538
- DOI: 10.1371/journal.pone.0055622
The impact of syphilis screening among female sex workers in China: a modelling study
Abstract
Background: In China, female sex workers (FSWs) are at high risk of syphilis infection, but are hard to reach for interventions. Point-of-care testing introduces opportunities for expanding syphilis control measures. Modelling is used to estimate the impact of using rapid tests to screen FSWs for syphilis. In other settings, modelling has predicted large rebounds in infectious syphilis following screening, which may undermine any impact achieved.
Methods: A deterministic syphilis transmission model among FSWs and clients was fitted to data from Yunnan Province (FSW syphilis prevalence = 7.5%), and used to estimate the impact of rapid syphilis testing and treatment for FSWs. Impact projections were compared for different model structures that included risk heterogeneity amongst FSWs, incoming syphilis infections amongst new FSWs and clients and re-infection from FSWs' regular non-commercial partners. The rebound in syphilis prevalence after screening ceased was explored.
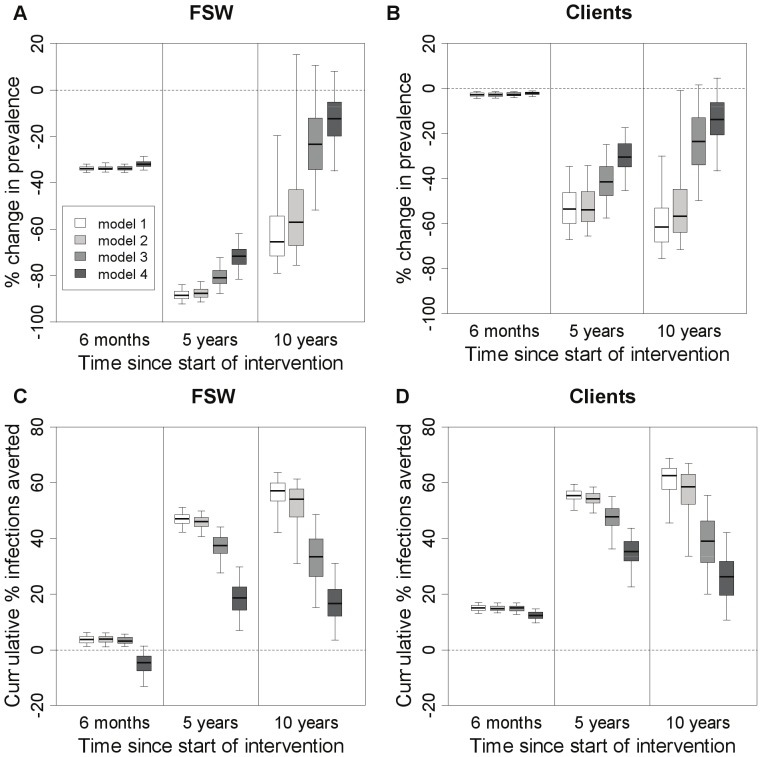
Results: All model structures suggest yearly syphilis screening could substantially reduce (by 72-88%) syphilis prevalence amongst FSWs in this setting over five years. However, incoming syphilis infections amongst new FSWs and clients or re-infections from regular non-commercial partners of FSWs can considerably reduce (>30%) the proportion of infections averted. Including heterogeneity in risk amongst FSWs had little effect upon the proportion of infections averted. In this setting, the rebound in syphilis prevalence after screening ceased is predicted to be slight, but it could be large in high prevalence settings.
Conclusions: Rapid test screening could dramatically reduce syphilis prevalence amongst hard-to-reach groups, but strategies to reduce re-infection from regular non-commercial partners are needed to maximise impact.
Conflict of interest statement
Figures
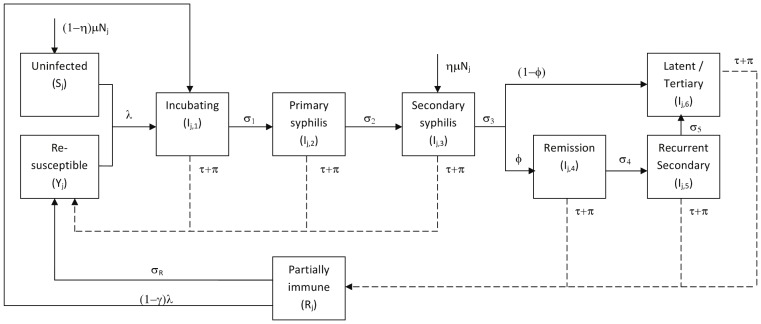
 leaving every compartment). Solid lines show normal transitions in the natural history, dashed lines show transitions due to treatment.
leaving every compartment). Solid lines show normal transitions in the natural history, dashed lines show transitions due to treatment.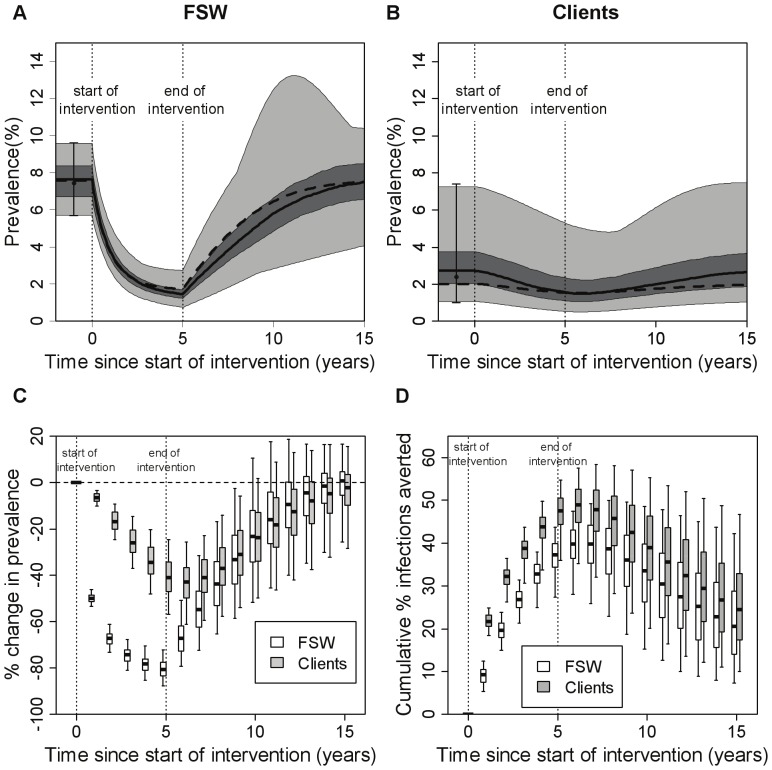
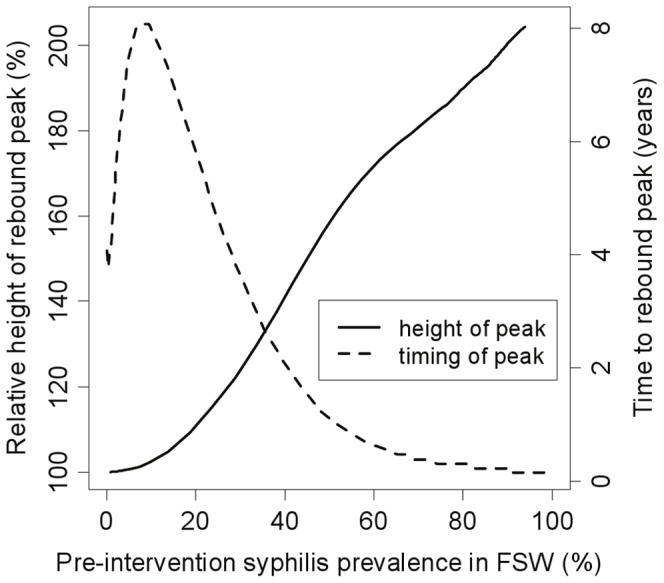
 (transmission probability per act) between 0.01 and 1 to produce different epidemic settings. A 5-year intervention with yearly testing of all FSWs, using a rapid test of 87% sensitivity, was simulated. The x-axis shows overall pre-intervention syphilis prevalence (all infected stages) in the FSW population (high risk+low risk), and the rebound statistics shown are for infectious syphilis (primary, secondary and recurrent secondary stages) in the total FSW population (high risk+low risk).
(transmission probability per act) between 0.01 and 1 to produce different epidemic settings. A 5-year intervention with yearly testing of all FSWs, using a rapid test of 87% sensitivity, was simulated. The x-axis shows overall pre-intervention syphilis prevalence (all infected stages) in the FSW population (high risk+low risk), and the rebound statistics shown are for infectious syphilis (primary, secondary and recurrent secondary stages) in the total FSW population (high risk+low risk).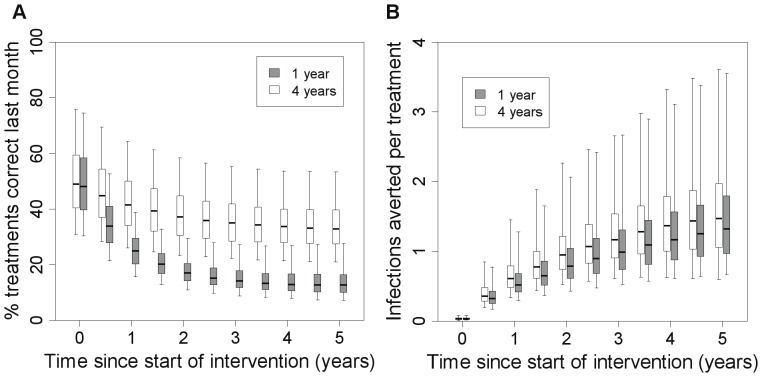
Similar articles
-
Declining Inconsistent Condom Use but Increasing HIV and Syphilis Prevalence Among Older Male Clients of Female Sex Workers: Analysis From Sentinel Surveillance Sites (2010-2015), Guangxi, China.Medicine (Baltimore). 2016 May;95(22):e3726. doi: 10.1097/MD.0000000000003726. Medicine (Baltimore). 2016. PMID: 27258500 Free PMC article.
-
A community-based comprehensive intervention to reduce syphilis infection among low-fee female sex workers in China: a matched-pair, community-based randomized study.Infect Dis Poverty. 2019 Dec 3;8(1):97. doi: 10.1186/s40249-019-0611-z. Infect Dis Poverty. 2019. PMID: 31791415 Free PMC article.
-
[A study on syphilis and HSV-2 infection and related behaviors among female sex workers who take new types of drugs in Jiaozhou city].Zhonghua Yu Fang Yi Xue Za Zhi. 2014 Oct;48(10):857-61. Zhonghua Yu Fang Yi Xue Za Zhi. 2014. PMID: 25573122 Chinese.
-
Prevalence of syphilis and chlamydia trachomatis infection among female sex workers in Jiangsu, China: Results from a multicenter cross-sectional and venue-based study.Front Public Health. 2022 Oct 31;10:1018724. doi: 10.3389/fpubh.2022.1018724. eCollection 2022. Front Public Health. 2022. PMID: 36388309 Free PMC article.
-
Syphilis among female sex workers in southwestern China: potential for HIV transmission.Sex Transm Dis. 2006 Dec;33(12):719-23. doi: 10.1097/01.olq.0000218881.01437.99. Sex Transm Dis. 2006. PMID: 16708055
Cited by
-
"I felt very small and embarrassed by the health care provider when I requested to be tested for syphilis": barriers and facilitators of regular syphilis and HIV testing among female sex workers in Uganda.BMC Public Health. 2021 Nov 2;21(1):1982. doi: 10.1186/s12889-021-12095-8. BMC Public Health. 2021. PMID: 34727898 Free PMC article.
-
High prevalence of syphilis among recyclable waste collectors in Central Brazil.Rev Soc Bras Med Trop. 2024 Feb 12;57:e007022024. doi: 10.1590/0037-8682-0283-2023. eCollection 2024. Rev Soc Bras Med Trop. 2024. PMID: 38359311 Free PMC article.
-
HIV and syphilis testing behaviors among heterosexual male and female sex workers in Uganda.AIDS Res Ther. 2020 Aug 1;17(1):48. doi: 10.1186/s12981-020-00306-y. AIDS Res Ther. 2020. PMID: 32738909 Free PMC article.
-
The introduction of syphilis point of care tests in resource limited settings.Expert Rev Mol Diagn. 2017 Apr;17(4):321-325. doi: 10.1080/14737159.2017.1303379. Epub 2017 Mar 14. Expert Rev Mol Diagn. 2017. PMID: 28266230 Free PMC article. Review.
-
Strategic options for syphilis control in Papua New Guinea- impact and cost-effectiveness projections using the syphilis interventions towards elimination (SITE) model.Infect Dis Model. 2021 Mar 20;6:584-597. doi: 10.1016/j.idm.2021.03.004. eCollection 2021. Infect Dis Model. 2021. PMID: 33869906 Free PMC article.
References
-
- Pirkle C, Soundardjee R, Stella A (2007) Female sex workers in China: vectors of disease.? Sex Transm Dis 34: 695–703. - PubMed
-
- van den Hoek A, Yuliang F, Dukers NH, Zhiheng C, Jiangting F, et al. (2001) High prevalence of syphilis and other sexually transmitted diseases among sex workers in China: potential for fast spread of HIV. AIDS 15: 753–759. - PubMed
-
- Lau JT, Tsui HY, Siah PC, Zhang KL (2002) A study on female sex workers in southern China (Shenzhen): HIV-related knowledge, condom use and STD history. AIDS Care 14: 219–233. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
