

Therapeutic application of melatonin in mild cognitive impairment
- PMID: 23383398
- PMCID: PMC3560473
Therapeutic application of melatonin in mild cognitive impairment
Abstract
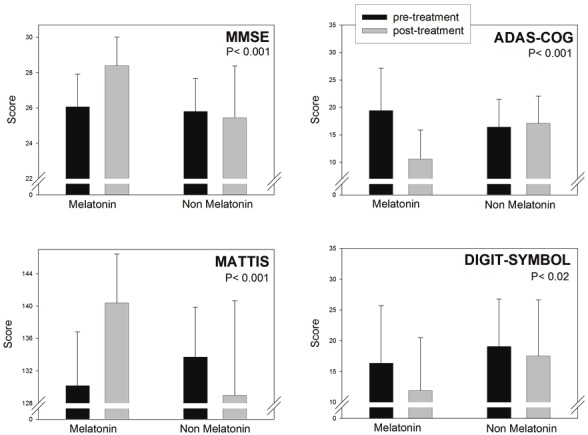
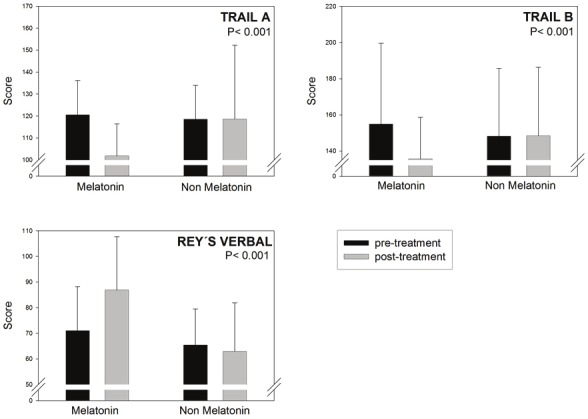
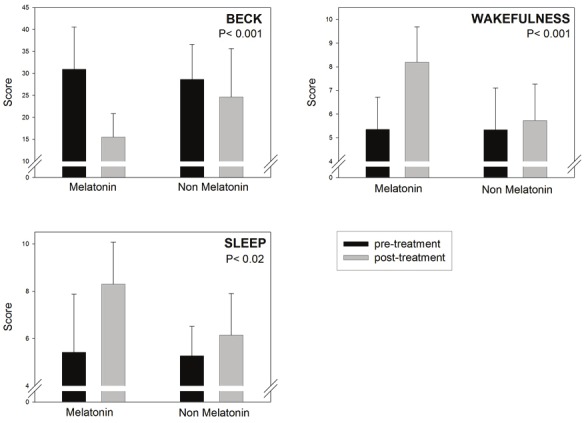
Mild cognitive impairment (MCI) is an etiologically heterogeneous syndrome defined by cognitive impairment in advance of dementia. We previously reported in a retrospective analysis that daily 3 - 9 mg of a fast-release melatonin preparation given p. o. at bedtime for up to 3 years significantly improved cognitive and emotional performance and daily sleep/wake cycle in MCI patients. In a follow up of that study we now report data from another series of 96 MCI outpatients, 61 of who had received daily 3 - 24 mg of a fast-release melatonin preparation p. o. at bedtime for 15 to 60 months. Melatonin was given in addition to the standard medication prescribed by the attending psychiatrist. Patients treated with melatonin exhibited significantly better performance in Mini-Mental State Examination and the cognitive subscale of the Alzheimer's disease Assessment Scale. After application of a neuropsychological battery comprising a Mattis´ test, Digit-symbol test, Trail A and B tasks and the Rey´s verbal test, better performance was found in melatonin-treated patients for every parameter tested. Abnormally high Beck Depression Inventory scores decreased in melatonin-treated patients, concomitantly with the improvement in the quality of sleep and wakefulness. The comparison of the medication profile in both groups of MCI patients indicated that 9.8% in the melatonin group received benzodiazepines vs. 62.8% in the non-melatonin group. The results further support that melatonin can be a useful add-on drug for treating MCI in a clinic environment.
Keywords: Alzheimer´s disease; Mild cognitive impairment; benzodiazepines; melatonin; neuropsychological tests; retrospective study.
Figures
References
-
- Silveri MC, Reali G, Jenner C, Puopolo M. Attention and memory in the preclinical stage of dementia. J Geriatr Psychiatry Neurol. 2007;20:67–75. - PubMed
-
- Weaver CJ, Maruff P, Collie A, Masters C. Mild memory impairment in healthy older adults is distinct from normal aging. Brain Cogn. 2006;60:146–155. - PubMed
-
- Grundman M, Petersen RC, Ferris SH, Thomas RG, Aisen PS, Bennett DA, Foster NL, Jack CR Jr, Galasko DR, Doody R, Kaye J, Sano M, Mohs R, Gauthier S, Kim HT, Jin S, Schultz AN, Schafer K, Mulnard R, van Dyck CH, Mintzer J, Zamrini EY, Cahn-Weiner D, Thal LJ. Mild cognitive impairment can be distinguished from Alzheimer disease and normal aging for clinical trials. Arch Neurol. 2004;61:59–66. - PubMed
-
- Dubois B, Albert ML. Amnestic MCI or prodromal Alzheimer's disease? Lancet Neurol. 2004;3:246–248. - PubMed
LinkOut - more resources
Full Text Sources