

Promoting work ability in a structured national rehabilitation program in patients with musculoskeletal disorders: outcomes and predictors in a prospective cohort study
- PMID: 23384339
- PMCID: PMC3626929
- DOI: 10.1186/1471-2474-14-57
Promoting work ability in a structured national rehabilitation program in patients with musculoskeletal disorders: outcomes and predictors in a prospective cohort study
Abstract
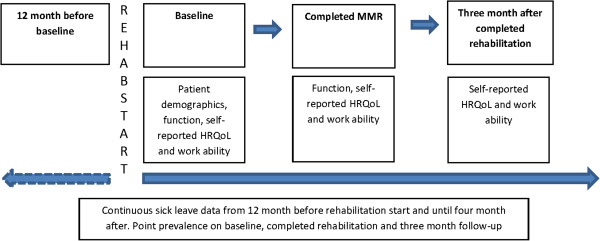
Background: Musculoskeletal disorders (MSDs) are a major reason for impaired work productivity and sick leave. In 2009, a national rehabilitation program was introduced in Sweden to promote work ability, and patients with MSDs were offered multimodal rehabilitation. The aim of this study was to analyse the effect of this program on health related quality of life, function, sick leave and work ability.
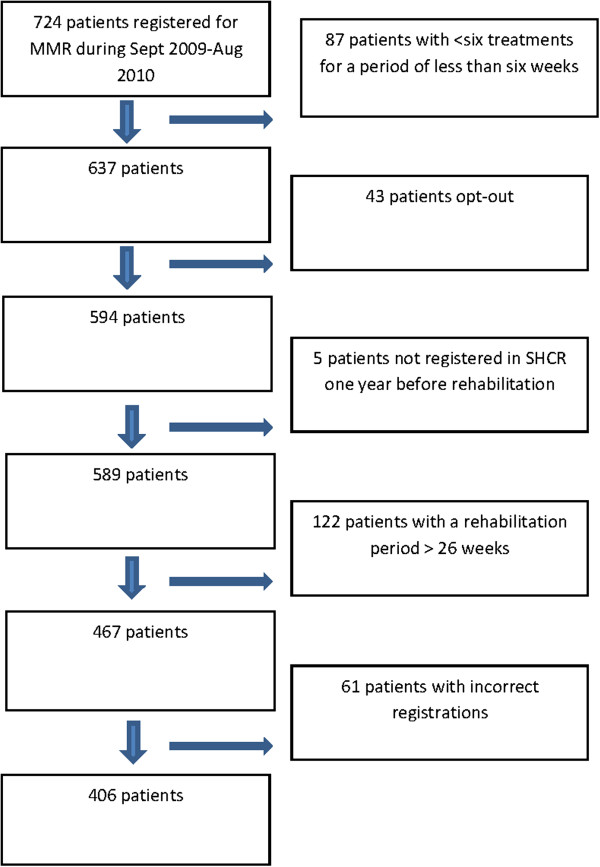
Methods: We conducted a prospective, observational cohort study including 406 patients with MSDs attending multimodal rehabilitation. Changes over time and differences between groups were analysed concerning function, health related quality of life, work ability and sick leave. Regression analyses were used to study the outcome variables health related quality of life (measured with EQ-5D), and sick leave.
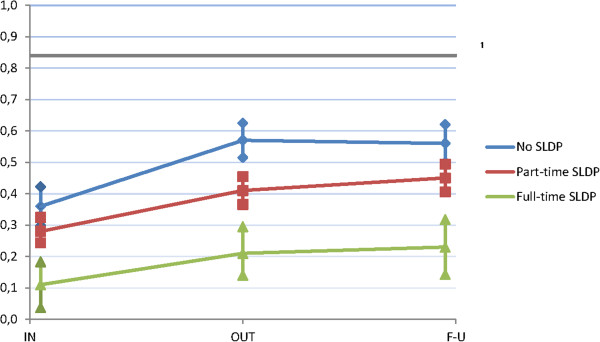
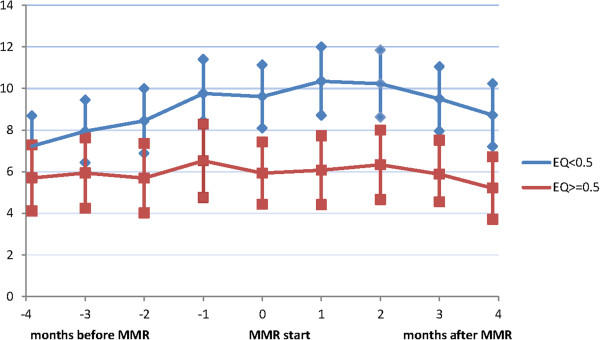
Results: Functional ability and health related quality of life improved after rehabilitation. Patients with no sick leave/disability pension the year before rehabilitation, improved health related quality of life more than patients with sick leave/disability pension the year before rehabilitation (p = 0.044). During a period of -/+ four months from rehabilitation start, patients with EQ-5D ≥ 0.5 at rehabilitation start, reduced their net sick leave days with 0.5 days and patients with EQ-5D <0.5 at rehabilitation start, increased net sick leave days with 1.5 days (p = 0.019). Factors negatively associated with sick leave at follow-up were earlier episodes of sick leave/disability pension, problems with exercise tolerance functions and mobility after rehabilitation. Higher age was associated with not being on sick leave at follow-up and reaching an EQ-5D ≥ 0.5 at follow-up. Severe pain after rehabilitation, problems with exercise tolerance functions, born outside of Sweden and full-time sick leave/disability pension the year before rehabilitation were all associated with an EQ-5D level < 0.5 at follow-up.
Conclusions: Patients with MSDs participating in a national work promoting rehabilitation program significantly improved their health related quality of life and functional ability, especially those with no sick leave. This shows that vocational rehabilitation programs in a primary health care setting are effective. The findings of this study can also be valuable for more appropriate patient selection for rehabilitation programs for MSDs.
Figures
References
-
- European Trade Union Institute (ETUI) Musculoskeletal disorders. An ill-understood pandemic. Brussel: ETUI; 2007. http://www.etui.org/Publications2/Guides/Musculoskeletal-disorders.-An-i....
-
- Beavan S, McGee R, Quadrello T. Fit for Work? Musculoskeletal Disorders and the Swedish Labour Market. The Work Foundation. Fit for work Europe. 2010. http://www.fitforworkeurope.eu/default.aspx.locid-0afnew00j.Lang-EN.htm.
-
- Lidwall U. Long-term Sickness Absence. Aspects of Society, Work and Family. Karolinska Institutet: Department of Clinical Neuroscience; 2010. (PhD-thesis). http://diss.kib.ki.se/2010/978-91-7409-821-1/thesis.pdf.
-
- Alexanderson K, Norlund A. Sickness absence- causes, consequences, and physicians’ certified sick leave practice. A systematic literature review by the Swedish council on technology assessments in health care. Scand J Publ Health. 2004;63(supplement):1–263. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
