

A simple immunohistochemical panel comprising 2 conventional markers, Ki67 and p53, is a powerful tool for predicting patient outcome in luminal-type breast cancer
- PMID: 23384409
- PMCID: PMC3577510
- DOI: 10.1186/1472-6890-13-5
A simple immunohistochemical panel comprising 2 conventional markers, Ki67 and p53, is a powerful tool for predicting patient outcome in luminal-type breast cancer
Abstract
Background: Ki67 is widely used in order to distinguish the "A" and "B" subtypes of luminal-type breast cancer. This study aimed to validate the prognostic value of adding p53 to Ki67 for characterizing luminal-type breast cancer.
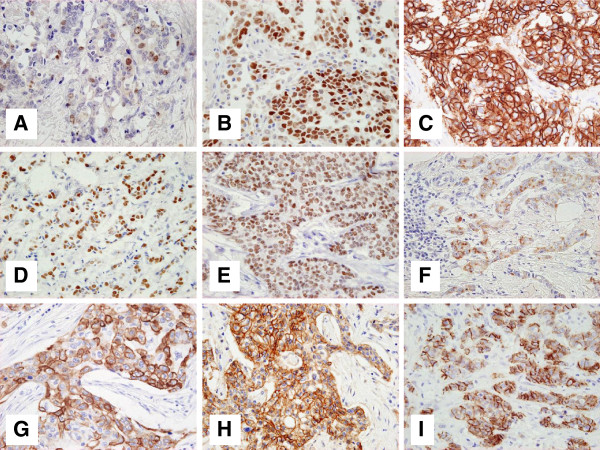
Methods: Immunostaining for Ki67, p53, and the molecular markers HER2, CK5/6, CK14, EGFR, FOXA1, GATA3, and P-cadherin was examined hormone receptor (HR)-positive cancer tissues from 150 patients. The prognostic value of an immunohistochemical panel comprising Ki67 and p53 was compared with that of the single Ki67 labeling index (LI), and uni- and multivariate analyses were performed.
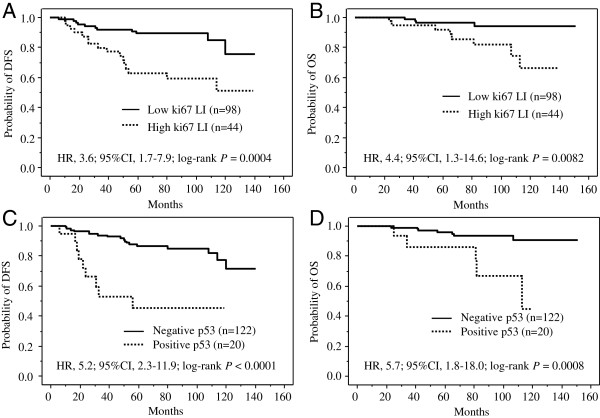
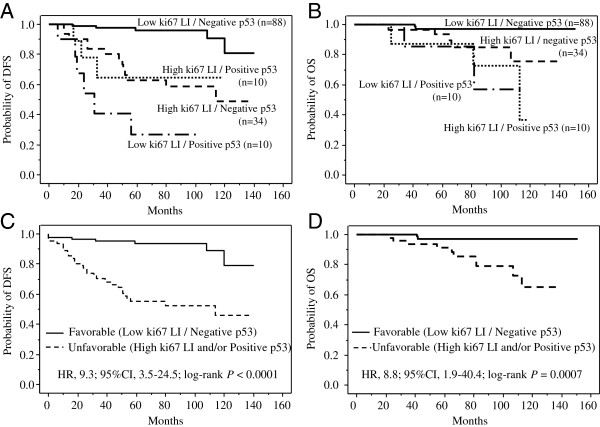
Results: Division of the patients based on the immunohistochemistry results into favorable- (low Ki67 LI, p53-negative) and unfavorable- (high Ki67 LI and/or p53-positive) phenotype groups yielded distinctly different Kaplan-Meier's curves of both disease-free (P<0.0001) and overall survival (P=0.0007). These differences were much more distinct than those between the corresponding low Ki67 LI vs. high Ki67LI curves. While the prognostic values of the other molecular markers were not significant, combined Ki67-p53 status was an independent prognostic factor by multivariate analysis.
Conclusion: These data indicate that an immunohistochemical panel comprising Ki67 and p53 is a practical tool for management of patients with HR-positive breast cancer.
Figures
References
-
- Early Breast Cancer Trialists' Collaborative Group. Tamoxifen for early breast cancer: an overview of the randomised trials. Lancet. 1998;351(9114):1451–1467. - PubMed
-
- Fisher B, Jeong JH, Bryant J, Anderson S, Dignam J, Fisher ER, Wolmark N. Treatment of lymph-node-negative, oestrogen-receptor-positive breast cancer: long-term findings from National Surgical Adjuvant Breast and Bowel Project randomised clinical trials. Lancet. 2004;364(9437):858–868. doi: 10.1016/S0140-6736(04)16981-X. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
