

Junctional spinal disorders in operated adult spinal deformities: present understanding and future perspectives
- PMID: 23386280
- PMCID: PMC3616458
- DOI: 10.1007/s00586-013-2676-x
Junctional spinal disorders in operated adult spinal deformities: present understanding and future perspectives
Abstract
Introduction: Junctional spinal disorders have become one of the greatest challenges in spinal deformity surgery. They can occur at any age but are mostly seen in adult deformity surgery and are most often observed as the patient gets older.
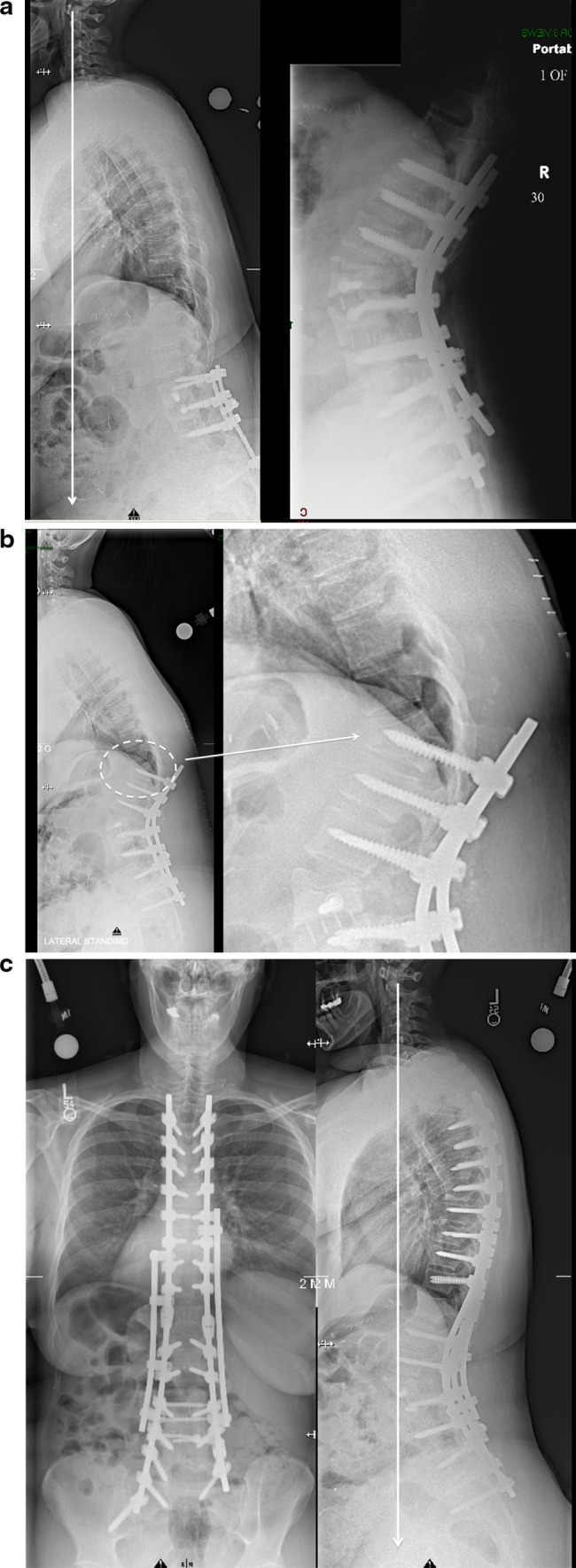
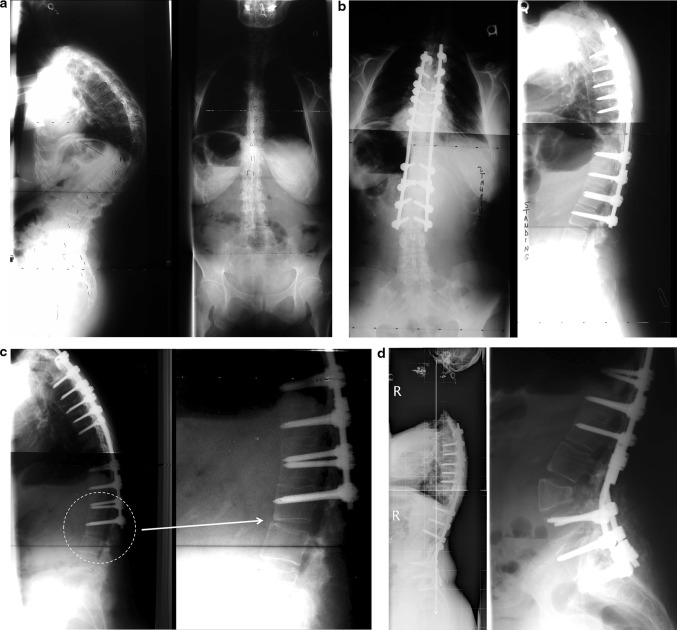
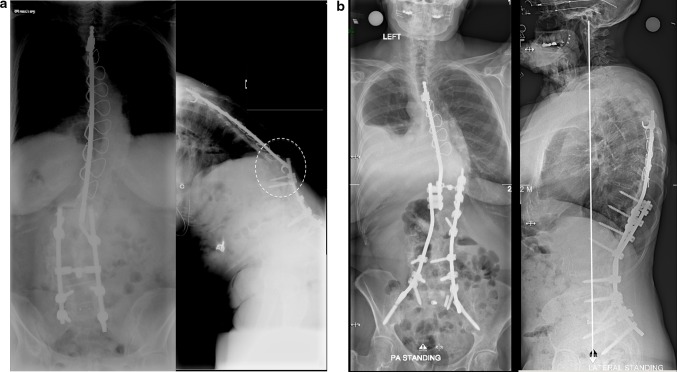
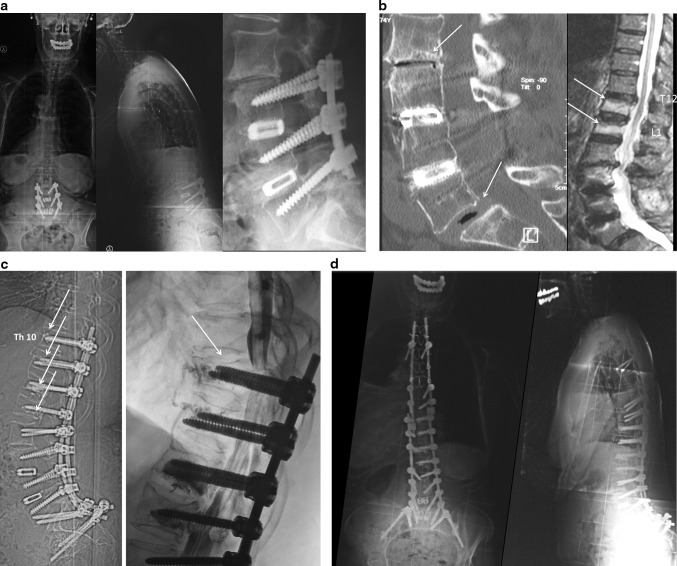
Definitions: Different forms can be individualized according to their types and location: one can observe simple segmental degeneration above or below instrumentation with or without spinal stenosis. Or the situation may be more complex with proximal junctional kyphosis, distal junctional kyphosis and intercalary junctional kyphosis where the junctional kyphosis occurs between two instrumented segments of the spine. Junctional scoliosis may also be observed as a new curve that did not exist after the index surgery.
Pathophysiology: Many different factors have been described being associated or the cause of junctional problems: old age, increased BMI, osteoporosis, etc. The role of pre-existing and postoperative sagittal imbalance plays a definitive role in their pathogenesis. As well the weakened posterior elements and or fatty degeneration of the posterior muscles are key factors in the occurrence of these problems. Multiple different radiologic parameters to describe and achieve perfect sagittal balance have been described knowing that the pelvic incidence of the patients is the key element that governs lumbar lordosis of the patient and hence the sagittal balance. Away from the spine one has to integrate the issues of the knees and the hips in the presentation of these junctional problems whether they are the cause or one of the consequences of the sagittal malalignment. Likewise the non-instrumented part of the spine (thoracic and or cervical spine) will also play a role in the pathogenesis or prevention of these junctional problems if they are stiff and or autofused along with their respective deformity.
Treatment: To prevent the occurrence of such junctional problems some basic surgical rules must be observed, but still lots remain unknown such as how much restoration of lordosis is really necessary, how to create a smoother transition between the instrumented and non-instrumented spine, which metal and where to use it, which implants to use as our widely used pedicle screw system may be one of the causes of these problems. Clinically these junctional problems can be asymptomatic and require only observation, or require revision surgery. Revision will require in most cases decompression of the neural elements, extension of the instrumentation and spinal osteotomies.
Conclusion: Definitively the issue of junctional spinal disorder after deformity surgery will require further extensive research to minimize this problem especially in our aging population.
Figures







References
-
- Schwab F, Dubey A, Gamez L, El Fegoun AB, Hwang K, Pagala M, Farcy JP. Adult scoliosis: prevalence, SF-36, and nutritional parameters in an elderly volunteer population. Spine. 2005;30(9):1082–1085. doi: 10.1097/01.brs.0000160842.43482.cd. - DOI - PubMed
-
- Hostin R, McCarthy I, O’Brien M, Bess S, Line B, Boachie-Adjei O, Burton D, Gupta M, Ames C, Deviren V, Kebaish K, Shaffrey C, Wood K, Hart R, International Spine Study Group (2012) Incidence, mode, and location of acute proximal junctional failures following surgical treatment for adult spinal deformity. Spine (Phila Pa 1976) [Epub ahead of print] - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
