

Endovascular treatment for acute ischemic stroke
- PMID: 23387822
- PMCID: PMC3708480
- DOI: 10.1056/NEJMoa1213701
Endovascular treatment for acute ischemic stroke
Abstract
Background: In patients with ischemic stroke, endovascular treatment results in a higher rate of recanalization of the affected cerebral artery than systemic intravenous thrombolytic therapy. However, comparison of the clinical efficacy of the two approaches is needed.
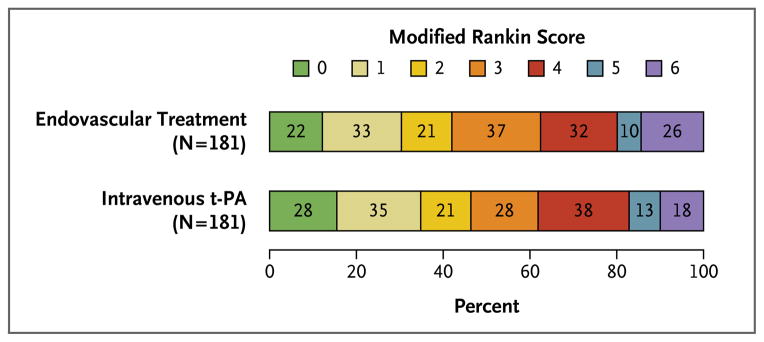
Methods: We randomly assigned 362 patients with acute ischemic stroke, within 4.5 hours after onset, to endovascular therapy (intraarterial thrombolysis with recombinant tissue plasminogen activator [t-PA], mechanical clot disruption or retrieval, or a combination of these approaches) or intravenous t-PA. Treatments were to be given as soon as possible after randomization. The primary outcome was survival free of disability (defined as a modified Rankin score of 0 or 1 on a scale of 0 to 6, with 0 indicating no symptoms, 1 no clinically significant disability despite symptoms, and 6 death) at 3 months.
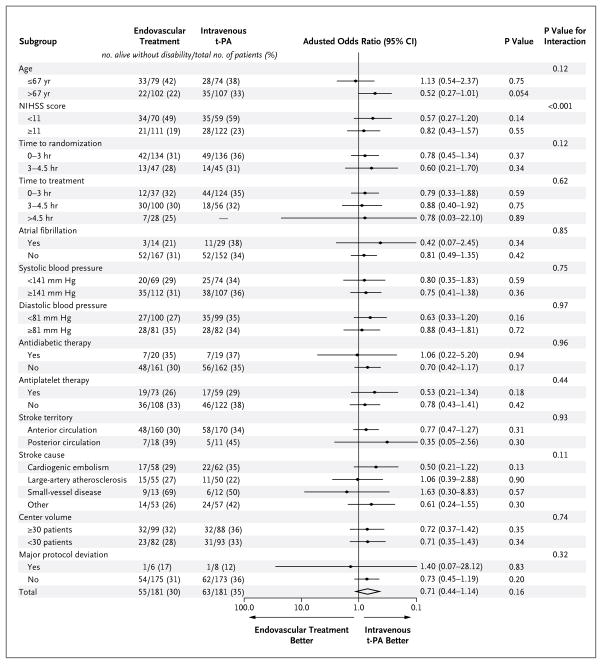
Results: A total of 181 patients were assigned to receive endovascular therapy, and 181 intravenous t-PA. The median time from stroke onset to the start of treatment was 3.75 hours for endovascular therapy and 2.75 hours for intravenous t-PA (P<0.001). At 3 months, 55 patients in the endovascular-therapy group (30.4%) and 63 in the intravenous t-PA group (34.8%) were alive without disability (odds ratio adjusted for age, sex, stroke severity, and atrial fibrillation status at baseline, 0.71; 95% confidence interval, 0.44 to 1.14; P=0.16). Fatal or nonfatal symptomatic intracranial hemorrhage within 7 days occurred in 6% of the patients in each group, and there were no significant differences between groups in the rates of other serious adverse events or the case fatality rate.
Conclusions: The results of this trial in patients with acute ischemic stroke indicate that endovascular therapy is not superior to standard treatment with intravenous t-PA. (Funded by the Italian Medicines Agency, ClinicalTrials.gov number, NCT00640367.).
Figures
Comment in
-
Endovascular treatment for acute ischemic stroke--still unproven.N Engl J Med. 2013 Mar 7;368(10):952-5. doi: 10.1056/NEJMe1215730. Epub 2013 Feb 8. N Engl J Med. 2013. PMID: 23394477 No abstract available.
-
[Is invasive therapy for stroke better than lysis? - time periods during stroke treatment have to be shortened].Dtsch Med Wochenschr. 2013 Apr;138(17):874-5. doi: 10.1055/s-0032-1329045. Epub 2013 Apr 16. Dtsch Med Wochenschr. 2013. PMID: 23592341 German. No abstract available.
-
Commentary: Societal statement on recent acute stroke intervention trials: results and implications.Neurosurgery. 2013 Aug;73(2):E375-9. doi: 10.1227/01.neu.0000430514.46473.4f. Neurosurgery. 2013. PMID: 23632768 No abstract available.
-
Endovascular treatment for acute ischemic stroke.N Engl J Med. 2013 Jun 20;368(25):2430-1. doi: 10.1056/NEJMc1304759. N Engl J Med. 2013. PMID: 23782184 No abstract available.
-
Endovascular treatment for acute ischemic stroke.N Engl J Med. 2013 Jun 20;368(25):2431. doi: 10.1056/NEJMc1304759. N Engl J Med. 2013. PMID: 23782185 No abstract available.
-
Endovascular treatment for acute ischemic stroke.N Engl J Med. 2013 Jun 20;368(25):2432. doi: 10.1056/NEJMc1304759. N Engl J Med. 2013. PMID: 23782187 No abstract available.
-
Endovascular treatment for acute ischemic stroke.N Engl J Med. 2013 Jun 20;368(25):2433-4. doi: 10.1056/NEJMc1304759. N Engl J Med. 2013. PMID: 23802240 No abstract available.
References
-
- del Zoppo GJ, Poeck K, Pessin MS, et al. Recombinant tissue plasminogen activator in acute thrombotic and embolic stroke. Ann Neurol. 1992;32:78–86. - PubMed
-
- Mazighi M, Serfaty JM, Labreuche J, et al. Comparison of intravenous alteplase with a combined intravenous-endovascular approach in patients with stroke and confirmed arterial occlusion (RECANALISE study): a prospective cohort study. Lancet Neurol. 2009;8:802–9. - PubMed
-
- Saqqur M, Uchino K, Demchuk AM, et al. Site of arterial occlusion identified by transcranial Doppler predicts the response to intravenous thrombolysis for stroke. Stroke. 2007;38:948–54. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical