

Safety of AS03-adjuvanted split-virion H1N1 (2009) pandemic influenza vaccine: a prospective cohort study
- PMID: 23388195
- PMCID: PMC3586178
- DOI: 10.1136/bmjopen-2012-001912
Safety of AS03-adjuvanted split-virion H1N1 (2009) pandemic influenza vaccine: a prospective cohort study
Erratum in
-
Correction.BMJ Open. 2013 Feb 19;3(2):e001912corr1. doi: 10.1136/bmjopen-2012-001912corr1. Print 2013. BMJ Open. 2013. PMID: 23427201 Free PMC article. No abstract available.
Abstract
Objectives: To assess the safety of an AS03-adjuvanted split virion H1N1 (2009) vaccine (Pandemrix) in persons vaccinated during the national pandemic influenza vaccination campaign in the UK.
Design: Prospective, cohort, observational, postauthorisation safety study.
Setting: 87 general practices forming part of the Medical Research Council General Practice Research Framework and widely distributed throughout England.
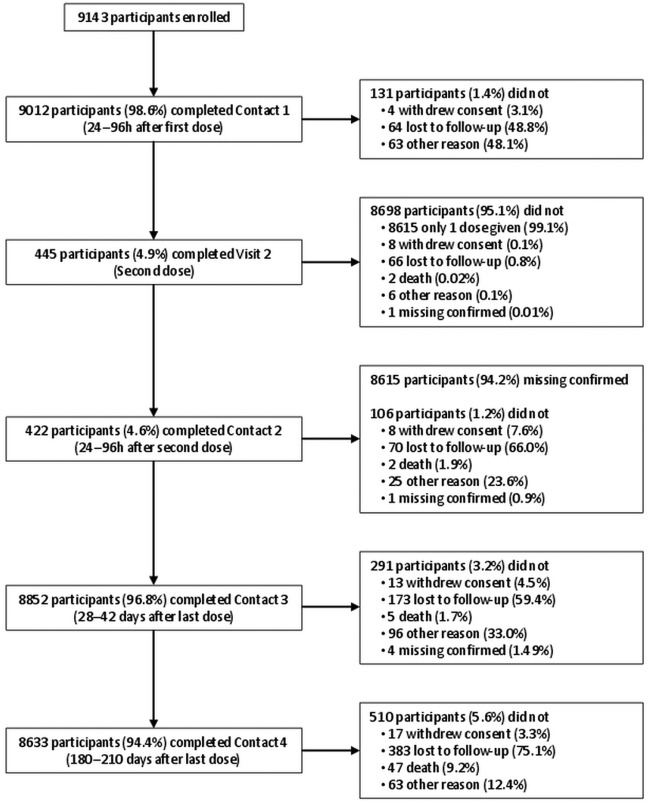
Participants: A cohort of 9143 individuals aged 7 months to 97 years who received at least one dose of the AS03-adjuvanted H1N1 pandemic vaccine during the national pandemic influenza vaccination campaign in the UK was enrolled. 94% completed the 6-month follow-up. Exclusion criteria were previous vaccination with other H1N1 pandemic vaccine and any child in care.
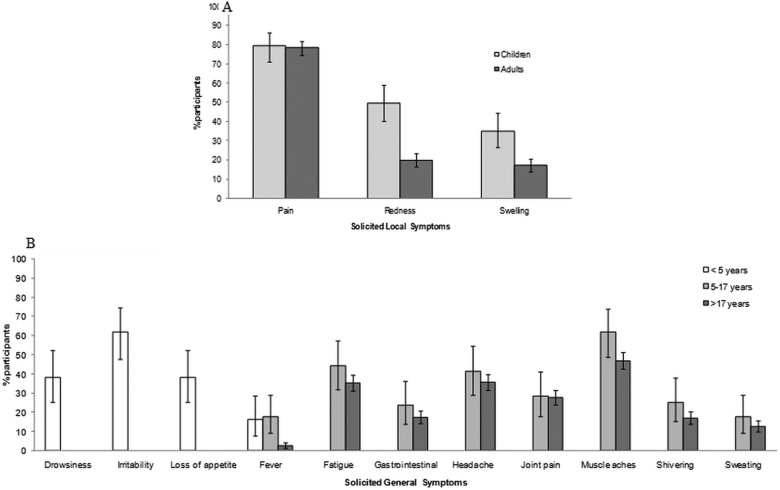
Primary and secondary outcome measures: Medically attended adverse events (MAEs) occurring within 31 days after any dose, serious adverse events (SAEs) and adverse events of special interest (AESIs) following vaccination were collected for all participants. Solicited adverse events (AEs) were assessed in a subset of participants.
Results: MAEs were reported in 1219 participants and SAEs in 113 participants during the 31-day postvaccination period. The most frequently reported MAEs and SAEs were consistent with events expected to be reported during the winter season in this population: lower respiratory tract infections, asthma and pneumonia. The most commonly reported solicited AEs were irritability in young children aged <5 years (61.8%), muscle aches in children aged 5-17 years (61.9%) and adults (46.9%). 18 AESIs, experienced by 14 patients, met the criteria to be considered for the observed-to-expected analyses. AESIs above the expected number were neuritis (1 case within 31 days) and convulsions (8 cases within 181 days). There were 41 deaths during the 181-day period after vaccination, fewer than expected.
Conclusions: Results indicate that the AS03-adjuvanted H1N1 pandemic vaccine showed a clinically acceptable reactogenicity and safety profile in all age and risk groups studied.
Trial registration: ClinicalTrials.gov, NCT00996853.
Figures
References
-
- Centers for Diseaes Control and Prevention (CDC) Update: novel influenza A (H1N1) virus infections—worldwide, May 6, 2009. MMWR Morb Mortal Wkly Rep 2009;58:453–8 - PubMed
-
- Centers for Disease Control and Prevention (CDC) Outbreak of swine-origin influenza A (H1N1) virus infection—Mexico, March-April 2009. MMWR Morb Mortal Wkly Rep 2009;58:467–70 - PubMed
-
- Centers for Disease Control and Prevention (CDC) Swine influenza A (H1N1) infection in two children—southern California, March-April 2009. MMWR Morb Mortal Wkly Rep 2009;58:400–2 - PubMed
-
- European Centre for Disease Prevention and Control ECDC Interim Guidance. Use of specific pandemic influenza vaccines during the H1N1 2009 pandemic. Aug 2009. European Centre for Disease Prevention and Control website. http://www.ecdc.europa.eu/en/publications/Publications/0908_GUI_Pandemic... (accessed 13 Apr 2012)
-
- National Center for Immunization and Respiratory Diseases (CDC), Centers for Disease Control and Prevention (CDC) Use of influenza A (H1N1) 2009 monovalent vaccine: recommendations of the Advisory Committee on Immunization Practices (ACIP), 2009. MMWR Recomm Rep 2009;58:1–8 - PubMed
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous