

Development of a genomic metric that can be rapidly used to predict clinical outcome in severely injured trauma patients
- PMID: 23388514
- PMCID: PMC3652285
- DOI: 10.1097/CCM.0b013e318277131c
Development of a genomic metric that can be rapidly used to predict clinical outcome in severely injured trauma patients
Abstract
Objective: Many patients have complicated recoveries following severe trauma due to the development of organ injury. Physiological and anatomical prognosticators have had limited success in predicting clinical trajectories. We report on the development and retrospective validation of a simple genomic composite score that can be rapidly used to predict clinical outcomes.
Design: Retrospective cohort study.
Setting: Multi-institutional level 1 trauma centers.
Patients: Data were collected from 167 severely traumatized (injury severity score >15) adult (18-55 yr) patients.
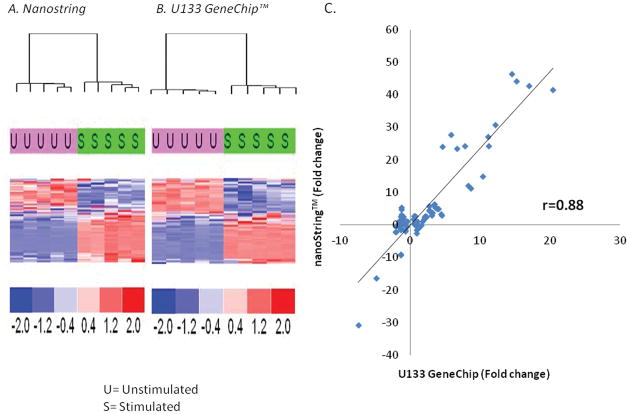
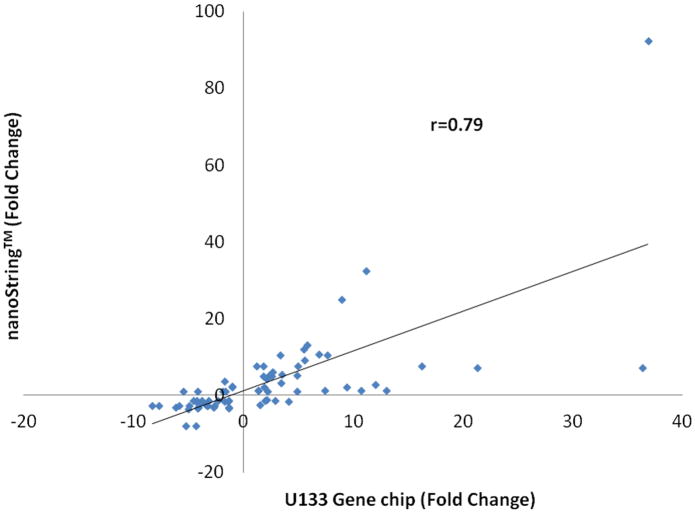
Methods: Microarray-derived genomic data obtained from 167 severely traumatized patients over 28 days were assessed for differences in messenger RNA abundance among individuals with different clinical trajectories. Once a set of genes was identified based on differences in expression over the entire study period, messenger RNA abundance from these subjects obtained in the first 24 hours was analyzed in a blinded fashion using a rapid multiplex platform, and genomic data reduced to a single metric.
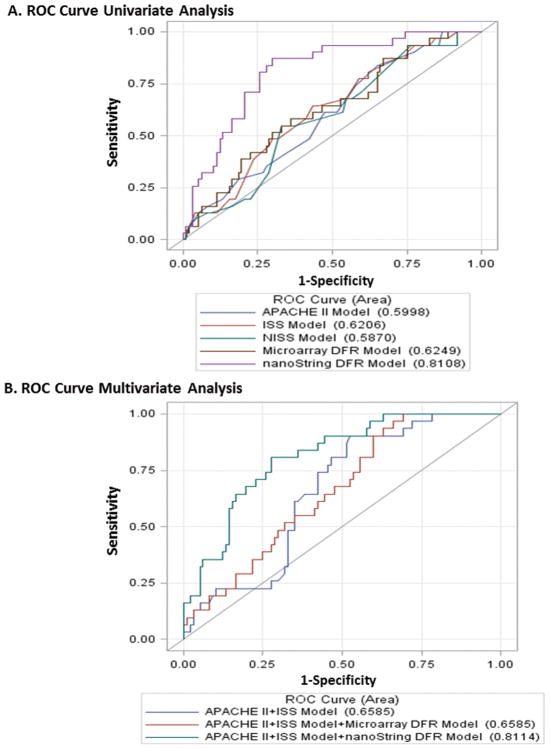
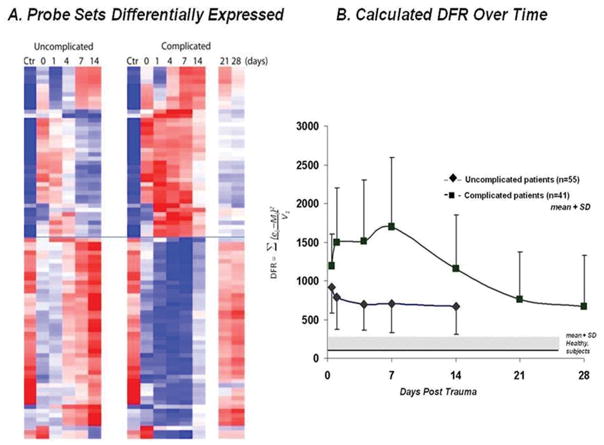
Results: From the existing genomic dataset, we identified 63 genes whose leukocyte expression differed between an uncomplicated and complicated clinical outcome over 28 days. Using a multiplex approach that can quantitate messenger RNA abundance in less than 12 hours, we reassessed total messenger RNA abundance from the first 24 hours after trauma and reduced the genomic data to a single composite score using the difference from reference. This composite score showed good discriminatory capacity to distinguish patients with a complicated outcome (area under a receiver-operator curve, 0.811; p <0.001). This was significantly better than the predictive power of either Acute Physiology and Chronic Health Evaluation II or new injury severity score scoring systems.
Conclusions: A rapid genomic composite score obtained in the first 24 hours after trauma can retrospectively identify trauma patients who are likely to develop complicated clinical trajectories. A novel platform is described in which this genomic score can be obtained within 12 hours of blood collection, making it available for clinical decision making.
Conflict of interest statement
The authors have not disclosed any potential conflicts of interest
Figures
Comment in
-
It's all in the genes: moving toward precision medicine in critical illness.Crit Care Med. 2013 May;41(5):1363-4. doi: 10.1097/CCM.0b013e31827c02dd. Crit Care Med. 2013. PMID: 23591214 No abstract available.
Similar articles
-
A genomic score prognostic of outcome in trauma patients.Mol Med. 2009 Jul-Aug;15(7-8):220-7. doi: 10.2119/molmed.2009.00027. Epub 2009 Apr 10. Mol Med. 2009. PMID: 19593405 Free PMC article.
-
Prediction of outcome in intensive care unit trauma patients: a multicenter study of Acute Physiology and Chronic Health Evaluation (APACHE), Trauma and Injury Severity Score (TRISS), and a 24-hour intensive care unit (ICU) point system.J Trauma. 1999 Aug;47(2):324-9. doi: 10.1097/00005373-199908000-00017. J Trauma. 1999. PMID: 10452468
-
[A new score system for prediction of death in patients with severe trauma: the value of death warning score].Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2015 Nov;27(11):890-4. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2015. PMID: 27132455 Chinese.
-
A comparison of the Acute Physiology and Chronic Health Evaluation (APACHE) II score and the Trauma-Injury Severity Score (TRISS) for outcome assessment in intensive care unit trauma patients.Crit Care Med. 1996 Oct;24(10):1642-8. doi: 10.1097/00003246-199610000-00007. Crit Care Med. 1996. PMID: 8874299
-
Comparison of the Sequential Organ Failure Assessment, Acute Physiology and Chronic Health Evaluation II scoring system, and Trauma and Injury Severity Score method for predicting the outcomes of intensive care unit trauma patients.Am J Emerg Med. 2012 Jun;30(5):749-53. doi: 10.1016/j.ajem.2011.05.022. Epub 2011 Jul 29. Am J Emerg Med. 2012. PMID: 21802884
Cited by
-
Systemic inflammation as a predictor of clinical outcomes after lower extremity angioplasty/stenting.J Vasc Surg. 2016 Sep;64(3):766-778.e5. doi: 10.1016/j.jvs.2015.04.399. Epub 2015 Jun 6. J Vasc Surg. 2016. PMID: 26054584 Free PMC article.
-
Breaking barriers in trauma research: A narrative review of opportunities to leverage veterinary trauma for accelerated translation to clinical solutions for pets and people.J Clin Transl Sci. 2024 Apr 5;8(1):e74. doi: 10.1017/cts.2024.513. eCollection 2024. J Clin Transl Sci. 2024. PMID: 38715566 Free PMC article. Review.
-
Unique transcriptomic response to sepsis is observed among patients of different age groups.PLoS One. 2017 Sep 8;12(9):e0184159. doi: 10.1371/journal.pone.0184159. eCollection 2017. PLoS One. 2017. PMID: 28886074 Free PMC article.
-
A Multidimensional Bioinformatic Platform for the Study of Human Response to Surgery.Ann Surg. 2022 Jun 1;275(6):1094-1102. doi: 10.1097/SLA.0000000000005429. Epub 2022 Mar 3. Ann Surg. 2022. PMID: 35258509 Free PMC article.
-
A better understanding of why murine models of trauma do not recapitulate the human syndrome.Crit Care Med. 2014 Jun;42(6):1406-13. doi: 10.1097/CCM.0000000000000222. Crit Care Med. 2014. PMID: 24413577 Free PMC article.
References
-
- Probst C, Pape HC, Hildebrand F, et al. 30 years of polytrauma care: An analysis of the change in strategies and results of 4849 cases treated at a single institution. Injury. 2009;40(1):77–83. - PubMed
-
- Cothren CC, Moore EE, Hedegaard HB, et al. Epidemiology of urban trauma deaths: a comprehensive reassessment 10 years later. World J Surg. 2007;31(7):1507–1511. - PubMed
-
- Bamvita JM, Bergeron E, Lavoie A, et al. The impact of premorbid conditions on temporal pattern and location of adult blunt trauma hospital deaths. J Trauma. 2007;63(1):135–141. - PubMed
-
- Demetriades D, Murray J, Charalambides K, et al. Trauma fatalities: time and location of hospital deaths. J Am Coll Surg. 2004;198(1):20–26. - PubMed
-
- Bone RC, Balk RA, Fein AM, et al. A second large controlled clinical study of E5, a monoclonal antibody to endotoxin: results of a prospective, multicenter, randomized, controlled trial. The E5 Sepsis Study Group. Crit Care Med. 1995;23(6):994–1006. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- R24 GM102656/GM/NIGMS NIH HHS/United States
- R01 GM104481/GM/NIGMS NIH HHS/United States
- U54 GM-062119-10/GM/NIGMS NIH HHS/United States
- P30 AG028740/AG/NIA NIH HHS/United States
- K23 GM087709/GM/NIGMS NIH HHS/United States
- F32 GM093665/GM/NIGMS NIH HHS/United States
- U54 GM062119/GM/NIGMS NIH HHS/United States
- K23 GM-087709-03/GM/NIGMS NIH HHS/United States
- F32 GM-093665-01/GM/NIGMS NIH HHS/United States
- T32 GM008721/GM/NIGMS NIH HHS/United States
- R01 GM101401/GM/NIGMS NIH HHS/United States
- R01 GM081923/GM/NIGMS NIH HHS/United States
- R01 GM040586/GM/NIGMS NIH HHS/United States
- T32 GM-008721-13/GM/NIGMS NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
