

Discovery and validation of cell cycle arrest biomarkers in human acute kidney injury
- PMID: 23388612
- PMCID: PMC4057242
- DOI: 10.1186/cc12503
Discovery and validation of cell cycle arrest biomarkers in human acute kidney injury
Abstract
Introduction: Acute kidney injury (AKI) can evolve quickly and clinical measures of function often fail to detect AKI at a time when interventions are likely to provide benefit. Identifying early markers of kidney damage has been difficult due to the complex nature of human AKI, in which multiple etiologies exist. The objective of this study was to identify and validate novel biomarkers of AKI.
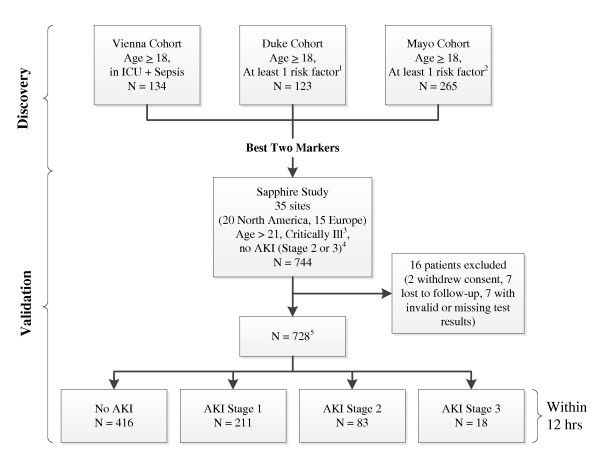
Methods: We performed two multicenter observational studies in critically ill patients at risk for AKI - discovery and validation. The top two markers from discovery were validated in a second study (Sapphire) and compared to a number of previously described biomarkers. In the discovery phase, we enrolled 522 adults in three distinct cohorts including patients with sepsis, shock, major surgery, and trauma and examined over 300 markers. In the Sapphire validation study, we enrolled 744 adult subjects with critical illness and without evidence of AKI at enrollment; the final analysis cohort was a heterogeneous sample of 728 critically ill patients. The primary endpoint was moderate to severe AKI (KDIGO stage 2 to 3) within 12 hours of sample collection.
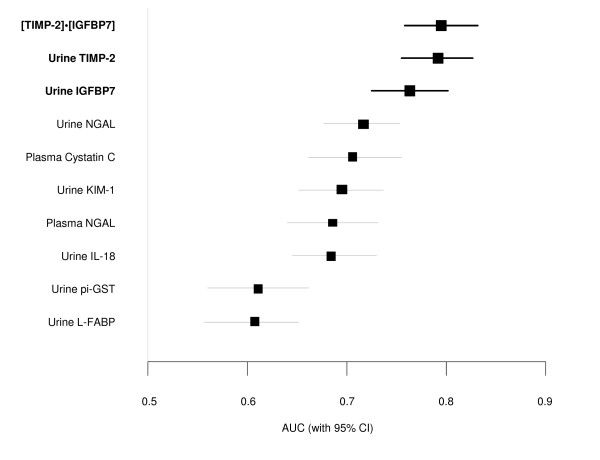
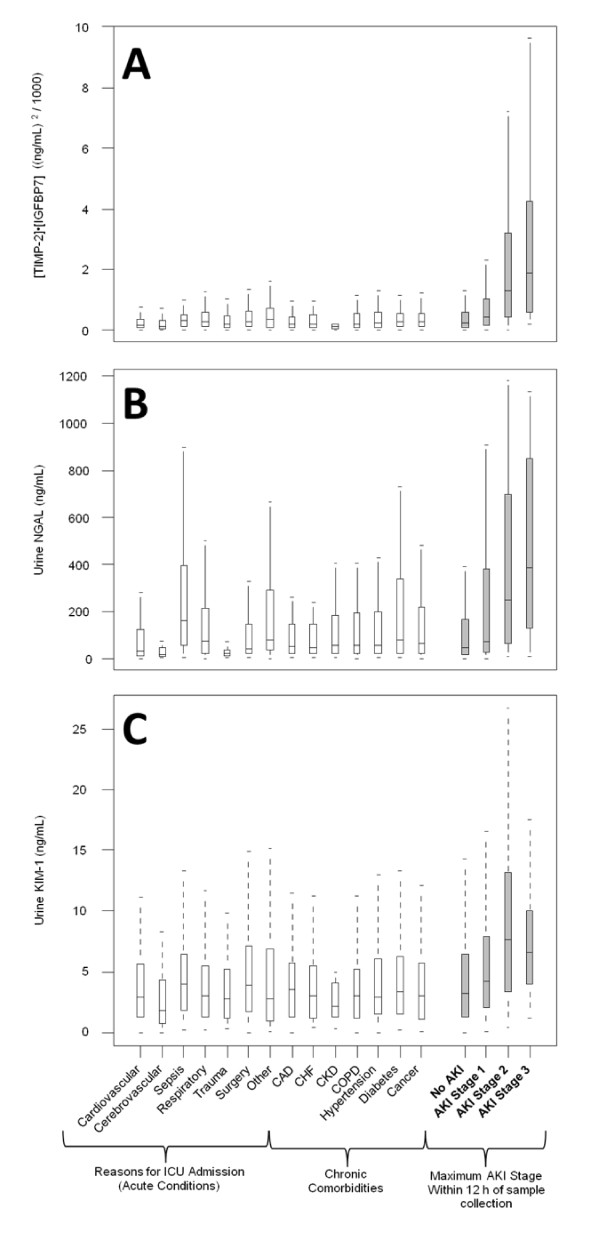
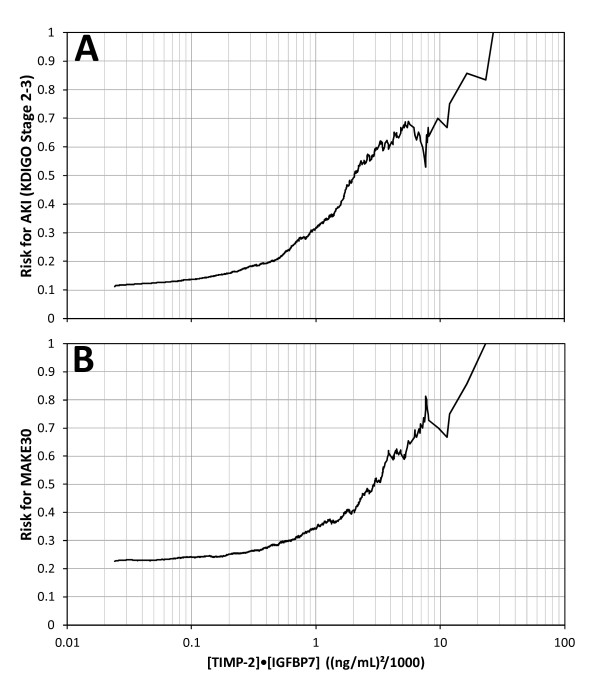
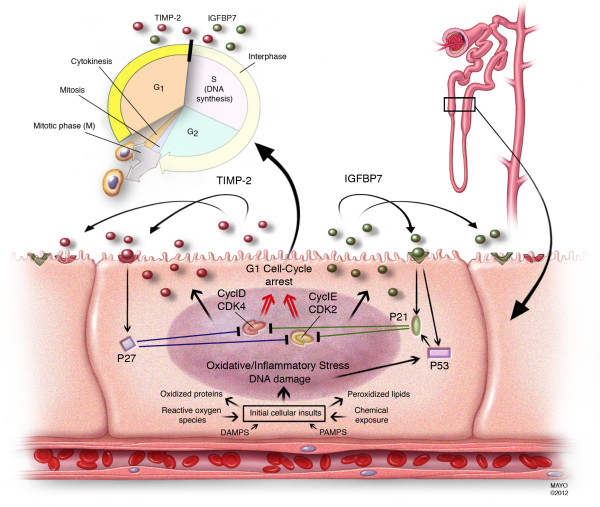
Results: Moderate to severe AKI occurred in 14% of Sapphire subjects. The two top biomarkers from discovery were validated. Urine insulin-like growth factor-binding protein 7 (IGFBP7) and tissue inhibitor of metalloproteinases-2 (TIMP-2), both inducers of G1 cell cycle arrest, a key mechanism implicated in AKI, together demonstrated an AUC of 0.80 (0.76 and 0.79 alone). Urine [TIMP-2]·[IGFBP7] was significantly superior to all previously described markers of AKI (P <0.002), none of which achieved an AUC >0.72. Furthermore, [TIMP-2]·[IGFBP7] significantly improved risk stratification when added to a nine-variable clinical model when analyzed using Cox proportional hazards model, generalized estimating equation, integrated discrimination improvement or net reclassification improvement. Finally, in sensitivity analyses [TIMP-2]·[IGFBP7] remained significant and superior to all other markers regardless of changes in reference creatinine method.
Conclusions: Two novel markers for AKI have been identified and validated in independent multicenter cohorts. Both markers are superior to existing markers, provide additional information over clinical variables and add mechanistic insight into AKI.
Trial registration: ClinicalTrials.gov number NCT01209169.
Figures
Comment in
-
The concept of risk and the value of novel markers of acute kidney injury.Crit Care. 2013 Feb 13;17(1):117. doi: 10.1186/cc12488. Crit Care. 2013. PMID: 23409754 Free PMC article.
References
-
- Kellum JA, Bellomo R, Ronco C. Kidney attack. JAMA. 2012;17:2265–2266. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
