

Confocal microscopy with strip mosaicing for rapid imaging over large areas of excised tissue
- PMID: 23389736
- PMCID: PMC3565124
- DOI: 10.1117/1.JBO.18.6.061227
Confocal microscopy with strip mosaicing for rapid imaging over large areas of excised tissue
Abstract
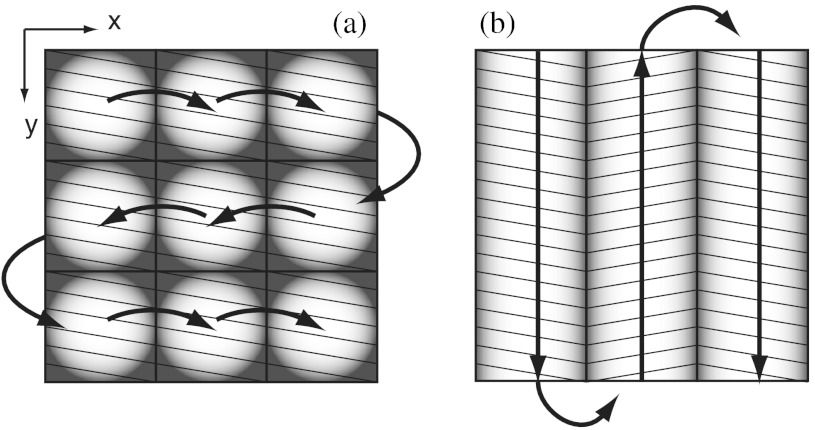
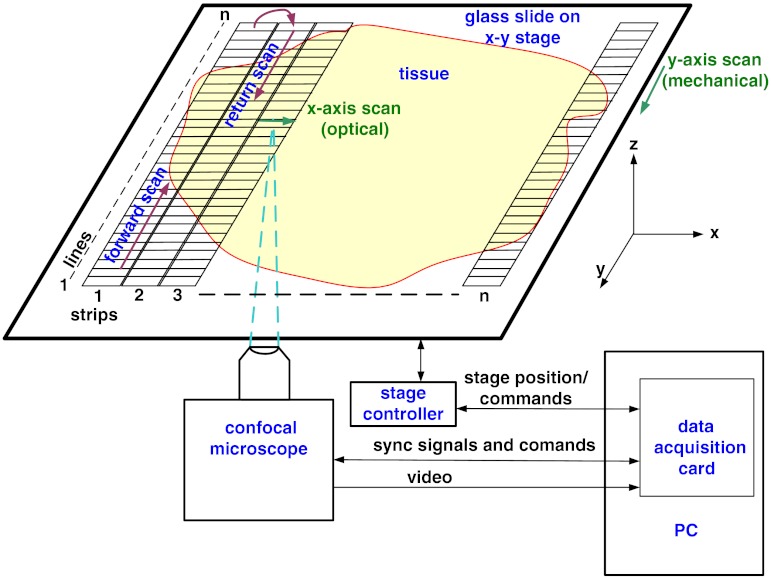
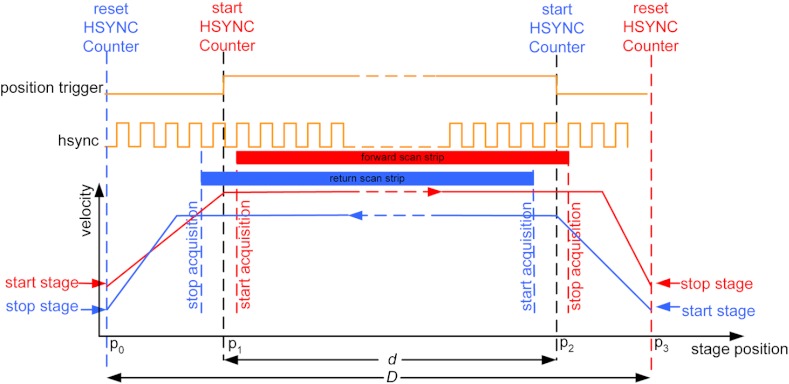
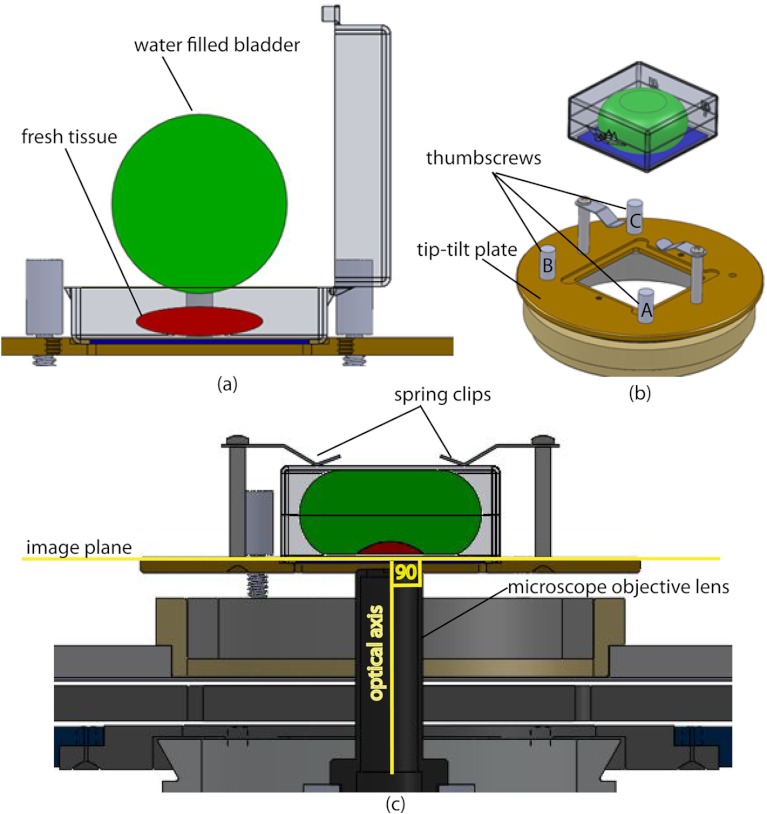
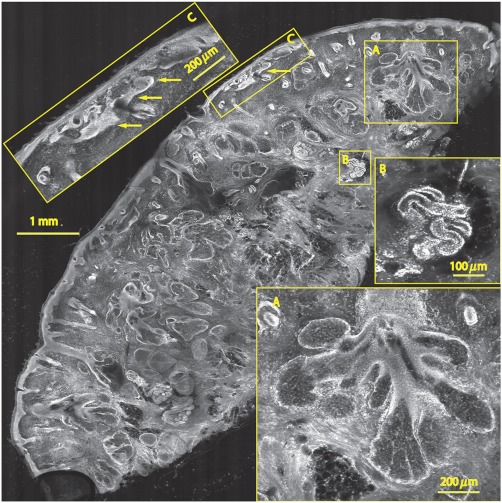
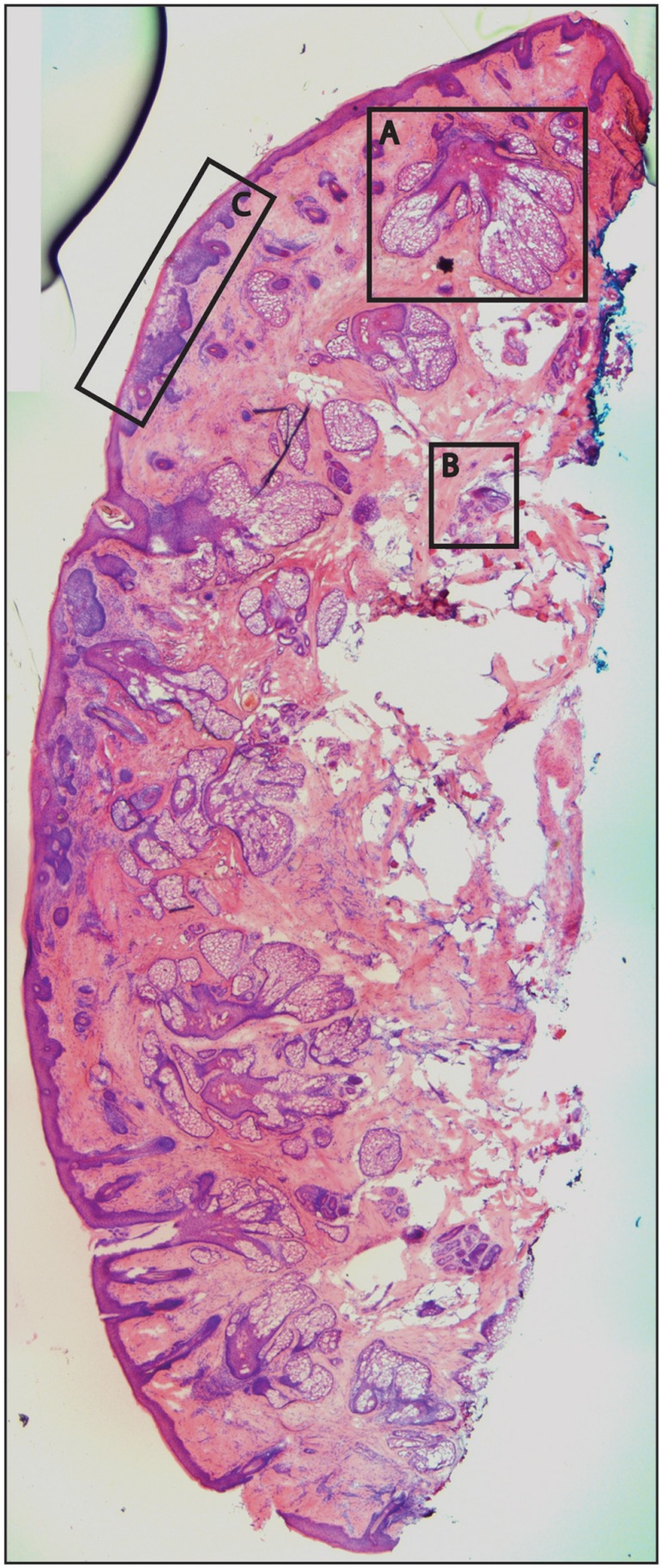
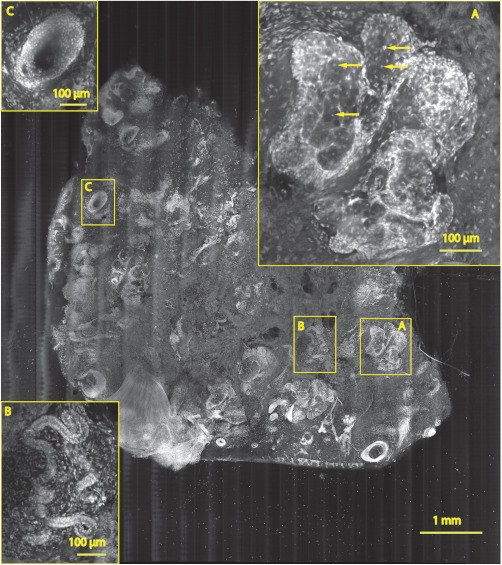
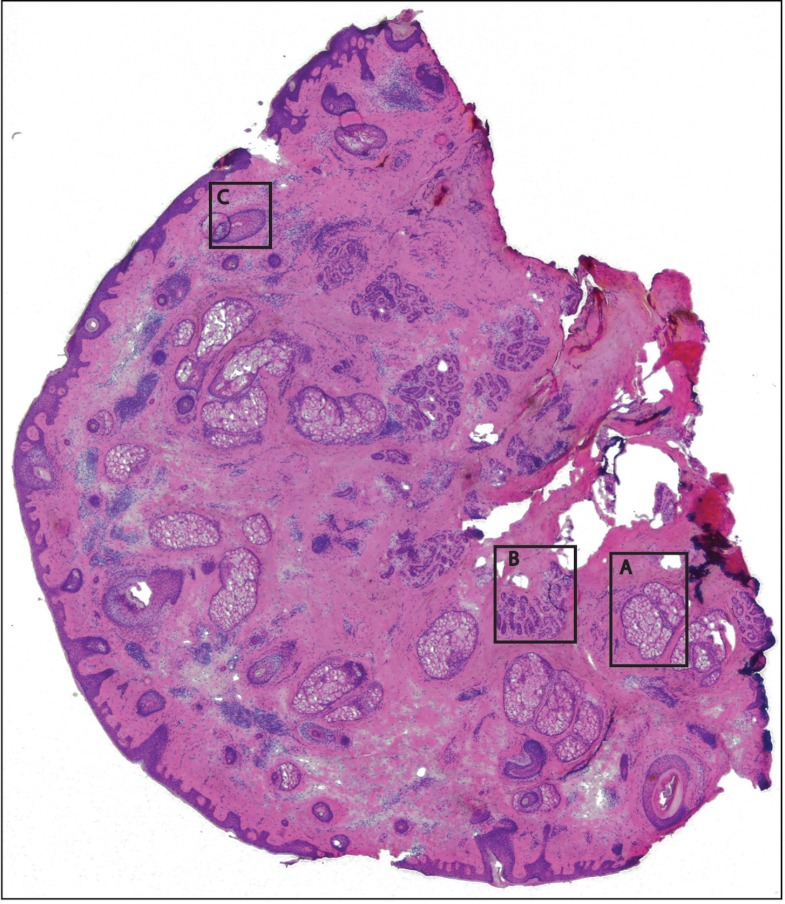
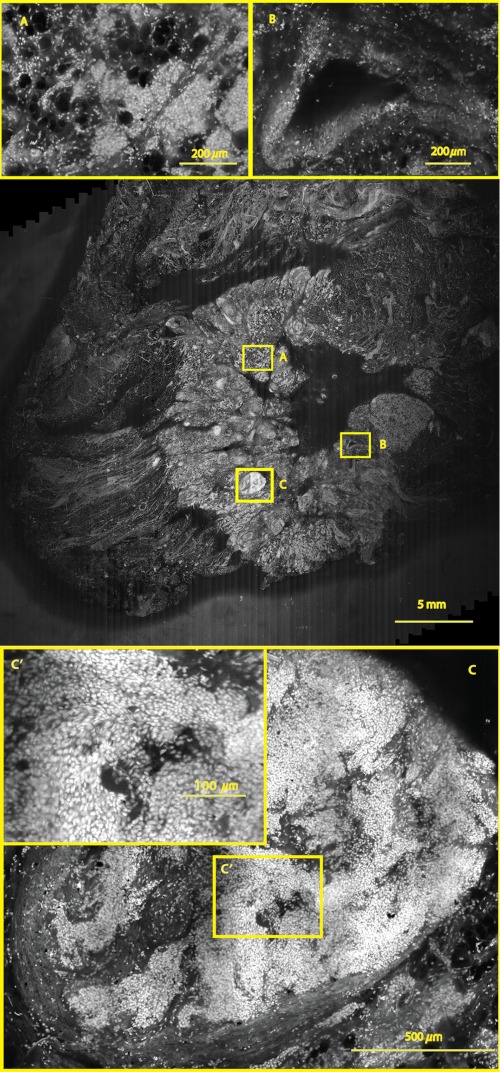
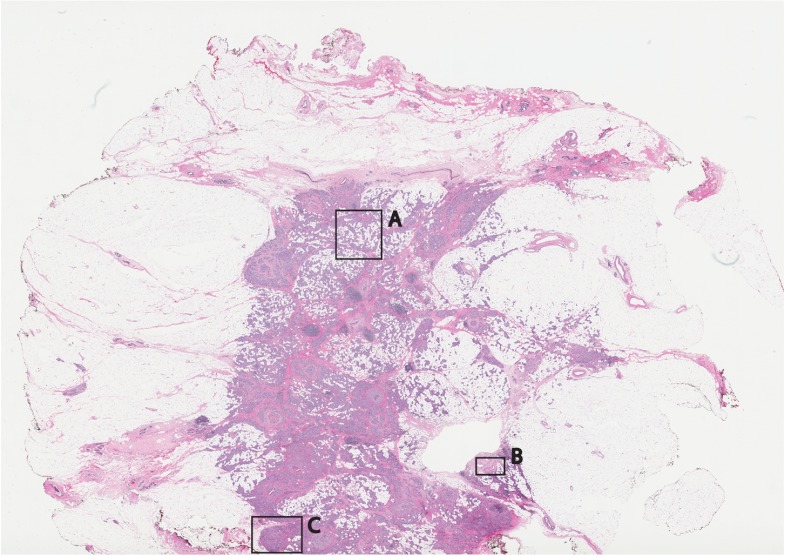
Confocal mosaicing microscopy is a developing technology platform for imaging tumor margins directly in freshly excised tissue, without the processing required for conventional pathology. Previously, mosaicing on 12-×-12 mm² of excised skin tissue from Mohs surgery and detection of basal cell carcinoma margins was demonstrated in 9 min. Last year, we reported the feasibility of a faster approach called "strip mosaicing," which was demonstrated on a 10-×-10 mm² of tissue in 3 min. Here we describe further advances in instrumentation, software, and speed. A mechanism was also developed to flatten tissue in order to enable consistent and repeatable acquisition of images over large areas. We demonstrate mosaicing on 10-×-10 mm² of skin tissue with 1-μm lateral resolution in 90 s. A 2.5-×-3.5 cm² piece of breast tissue was scanned with 0.8-μm lateral resolution in 13 min. Rapid mosaicing of confocal images on large areas of fresh tissue potentially offers a means to perform pathology at the bedside. Imaging of tumor margins with strip mosaicing confocal microscopy may serve as an adjunct to conventional (frozen or fixed) pathology for guiding surgery.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
