

Role of procoagulant microparticles in mediating complications and outcome of acute liver injury/acute liver failure
- PMID: 23389887
- PMCID: PMC5571831
- DOI: 10.1002/hep.26307
Role of procoagulant microparticles in mediating complications and outcome of acute liver injury/acute liver failure
Abstract
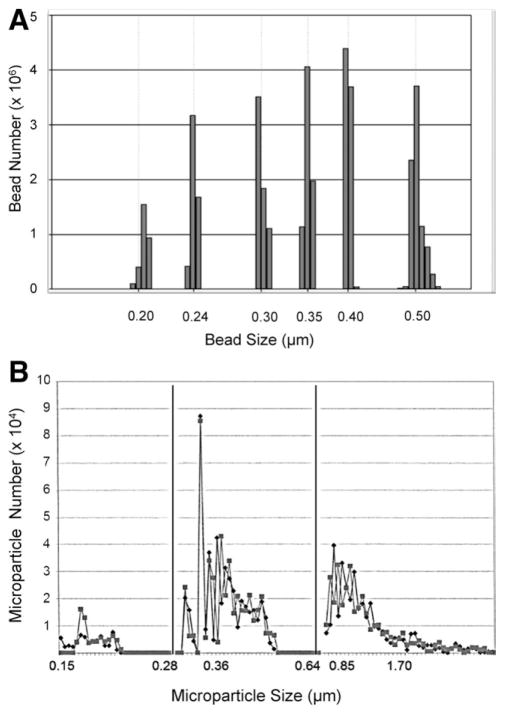
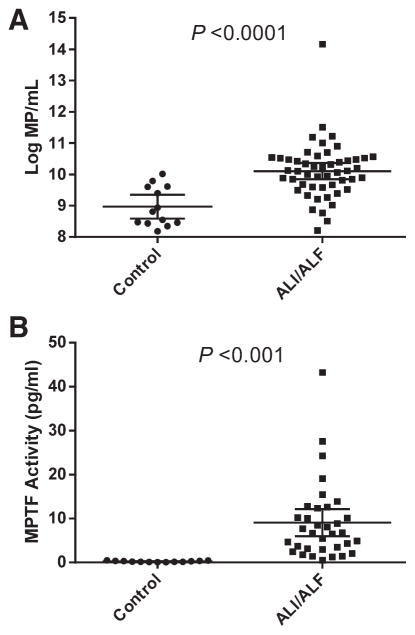
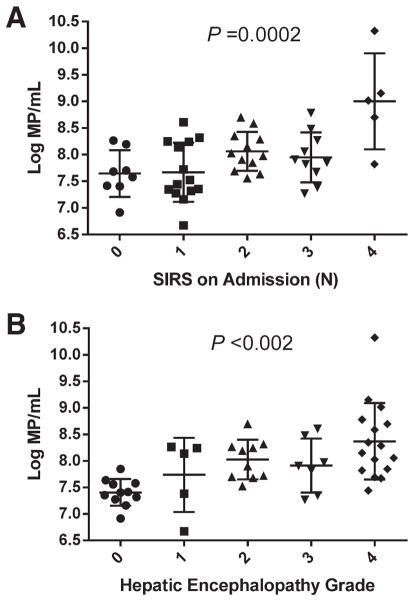
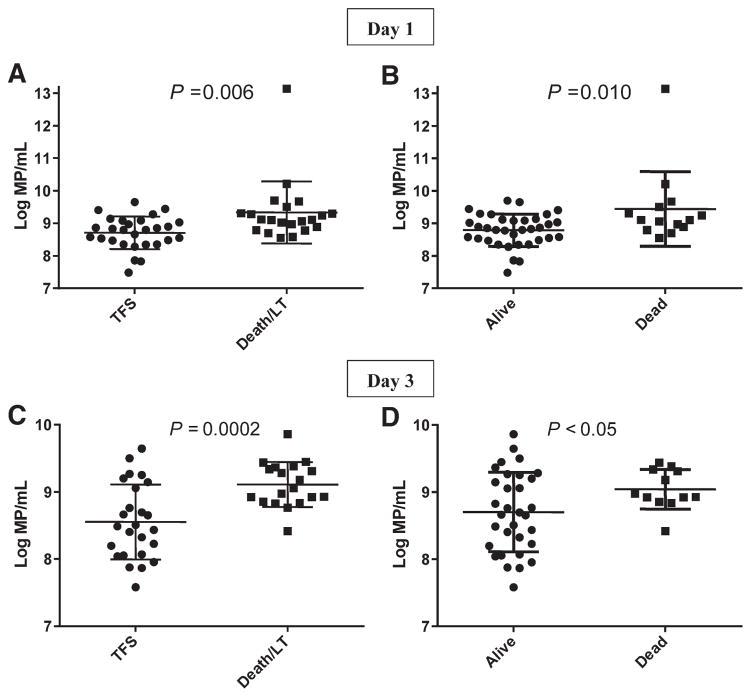
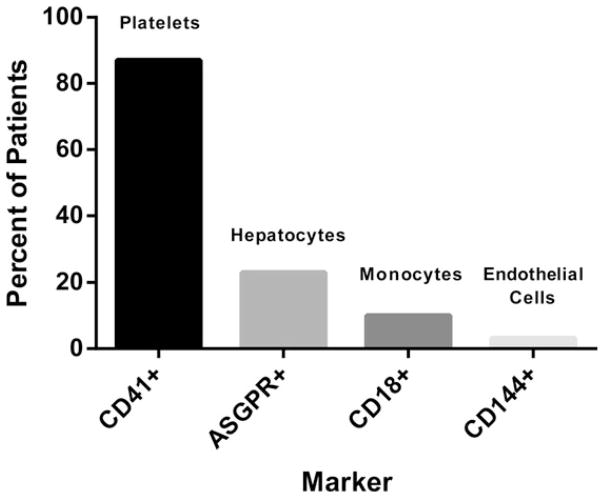
Microparticles (MPs), membrane fragments of 0.1-1.0 μm, are derived from many cell types in response to systemic inflammation. Acute liver failure (ALF) is a prototypical syndrome of systemic inflammatory response syndrome (SIRS) associated with a procoagulant state. We hypothesized that patients with ALF develop increased procoagulant MPs in proportion to the severity of systemic complications and adverse outcome. Fifty patients with acute liver injury (ALI), 78% of whom also had hepatic encephalopathy (HE; ALF), were followed until day 21 after admission. MPs were characterized by Invitrox Sizing, Antigen Detection and Enumeration, a light-scattering technology that can enumerate MPs as small as 0.15 μm, and by flow cytometry. Procoagulant activity was assessed by a functional MP-tissue factor (MP-TF) assay. Sixteen patients (32%) died and 27 (54%) recovered without liver transplantation (LT). Total MPs (0.15-1.0 μm) were present in nearly 19-fold higher concentrations in ALI/ALF patients, compared to healthy controls (P < 0.0001). MP-TF assays revealed high procoagulant activity (9.05 ± 8.82 versus 0.24 ± 0.14 pg/mL in controls; P = 0.0008). MP concentrations (0.28-0.64 μm) were higher in patients with the SIRS and high-grade HE, and MPs in the 0.36-0.64-μm size range increased in direct proportion to SIRS severity (P < 0.001) and grade of HE (P < 0.002). Day 1 MPs (0.28-0.64 μm) correlated with laboratory predictors of death/LT (higher phosphate and creatinine; lower bicarbonate), and day 1 and 3 MPs were higher in patients who died or underwent LT, compared to spontaneous survivors (P ≤ 0.01). By flow cytometry, 87% of patients had circulating CD41(+) MPs, indicating platelet origin.
Conclusion: Highly procoagulant MPs of specific size ranges are associated with the SIRS, systemic complications, and adverse outcome of ALI/ALF. MPs may contribute to the multiorgan system failure and high mortality of ALF.
Copyright © 2013 American Association for the Study of Liver Diseases.
Conflict of interest statement
Potential conflict of interest: D.A.G. acknowledges his role as Chief Medical Officer of Invitrox, Inc. The focus of Invitrox is to develop new technology to detect and phenotype microparticles and to explore potential clinical applications of this technology.
Figures
References
-
- Bernal W, Auzinger G, Sizer E, Wendon J. Intensive care management of acute liver failure. Semin Liver Dis. 2008;28:188–200. - PubMed
-
- Rolando N, Wade J, Davalos M, Wendon J, Philpott-Howard J, Williams R. The systemic inflammatory response syndrome in acute liver failure. Hepatology. 2000;32:734–739. - PubMed
-
- Stravitz RT, Kramer DJ. Management of acute liver failure. Nat Rev Gastroenterol Hepatol. 2009;6:542–553. - PubMed
-
- Antoniades CG, Berry PA, Wendon JA, Vergani D. The importance of immune dysfunction in determining outcome in acute liver failure. J Hepatol. 2008;49:845–861. - PubMed
-
- Munoz SJ, Stravitz RT, Gabriel DA. Coagulopathy of acute liver failure. Clin Liver Dis. 2009;13:95–107. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous