

The Stroop smartphone application is a short and valid method to screen for minimal hepatic encephalopathy
- PMID: 23389962
- PMCID: PMC3657327
- DOI: 10.1002/hep.26309
The Stroop smartphone application is a short and valid method to screen for minimal hepatic encephalopathy
Abstract
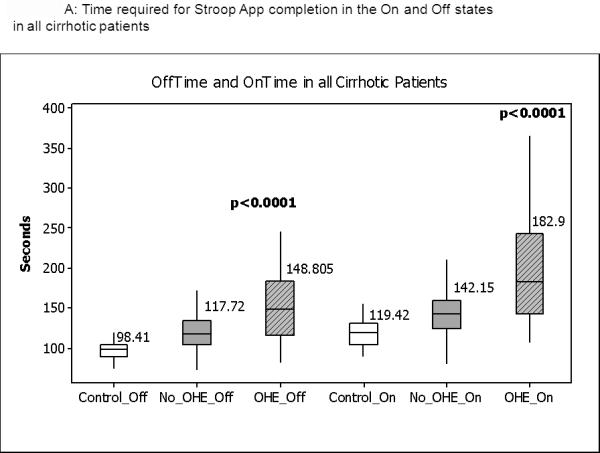
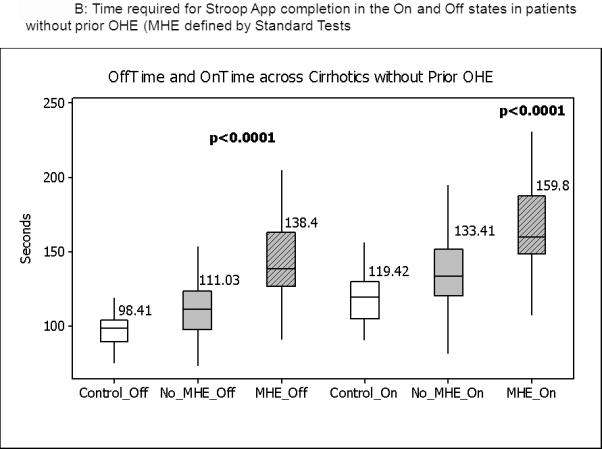
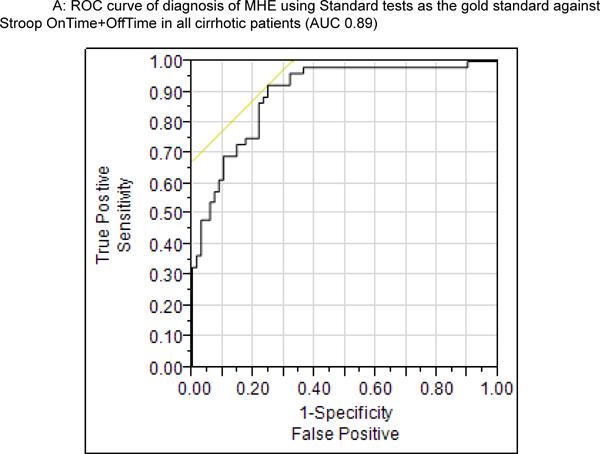
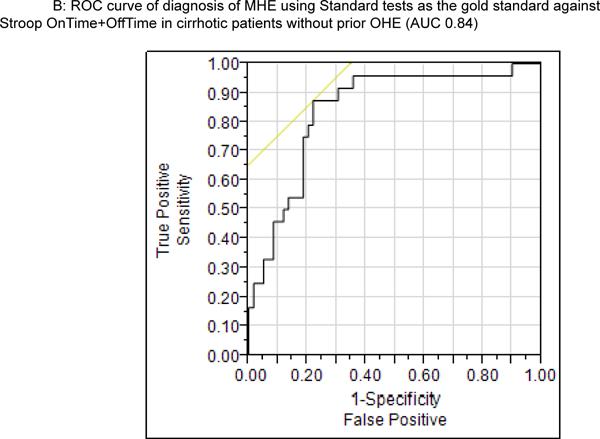
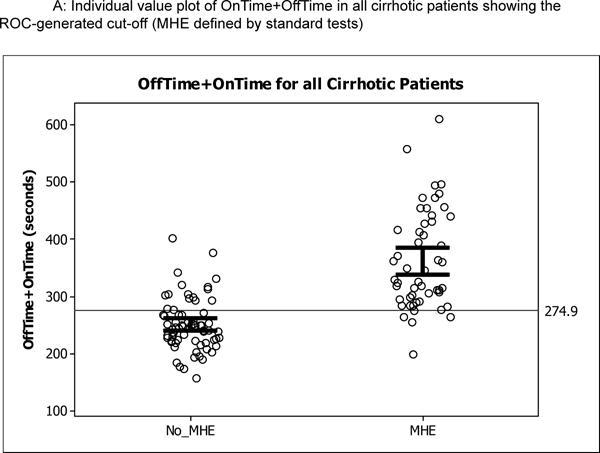
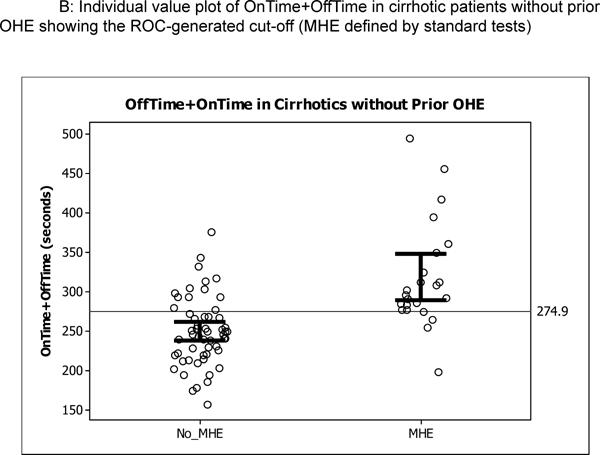
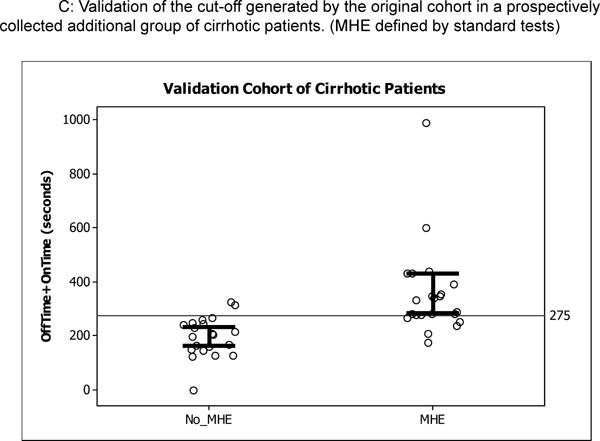
Minimal hepatic encephalopathy (MHE) detection is difficult because of the unavailability of short screening tools. Therefore, MHE patients can remain undiagnosed and untreated. The aim of this study was to use a Stroop smartphone application (app) (EncephalApp_Stroop) to screen for MHE. The app and standard psychometric tests (SPTs; 2 of 4 abnormal is MHE, gold standard), psychometric hepatic encephalopathy score (PHES), and inhibitory control tests (ICTs) were administered to patients with cirrhosis (with or without previous overt hepatic encephalopathy; OHE) and age-matched controls from two centers; a subset underwent retesting. A separate validation cohort was also recruited. Stroop has an "off" state with neutral stimuli and an "on" state with incongruent stimuli. Outcomes included time to complete five correct runs as well as number of trials needed in on (Ontime) and off (Offtime) states. Stroop results were compared between controls and patients with cirrhosis with or without OHE and those with or without MHE (using SPTs, ICTs, and PHES). Receiver operating characteristic analysis was performed to diagnose MHE in patients with cirrhosis with or without previous OHE. One hundred and twenty-five patients with cirrhosis (43 previous OHE) and 134 controls were included in the original cohort. App times were correlated with Model for End-Stage Liver Disease (Offtime: r = 0.57; Ontime: r = 0.61; P < 0.0001) and were worst in previous OHE patients, compared to the rest and controls. Stroop performance was also significantly impaired in those with MHE, compared to those without MHE, according to SPTs, ICTs, and PHES (all P < 0.0001). A cutoff of >274.9 seconds (Ontime plus Offtime) had an area under the curve of 0.89 in all patients and 0.84 in patients without previous OHE for MHE diagnosis using SPT as the gold standard. The validation cohort showed 78% sensitivity and 90% specificity with the >274.9-seconds Ontime plus Offtime cutoff. App result patterns were similar between the centers. Test-retest reliability in controls and those without previous OHE was good; a learning effect on Ontime in patients with cirrhosis without previous OHE was noted.
Conclusion: The Stroop smartphone app is a short, valid, and reliable tool for screening of MHE.
Copyright © 2013 American Association for the Study of Liver Diseases.
Figures
Comment in
-
Smart applications for assessing minimal hepatic encephalopathy: novelty from the app revolution.Hepatology. 2013 Sep;58(3):844-6. doi: 10.1002/hep.26416. Epub 2013 Jul 29. Hepatology. 2013. PMID: 23532934 No abstract available.
References
-
- Ferenci P, Lockwood A, Mullen K, Tarter R, Weissenborn K, Blei AT. Hepatic encephalopathy--definition, nomenclature, diagnosis, and quantification: final report of the working party at the 11th World Congresses of Gastroenterology, Vienna, 1998. Hepatology. 2002;35:716–721. - PubMed
-
- Bajaj JS, Wade JB, Sanyal AJ. Spectrum of neurocognitive impairment in cirrhosis: Implications for the assessment of hepatic encephalopathy. Hepatology. 2009;50:2014–2021. - PubMed
-
- Ortiz M, Jacas C, Cordoba J. Minimal hepatic encephalopathy: diagnosis, clinical significance and recommendations. J Hepatol. 2005;42(Suppl):S45–53. - PubMed
-
- Soriano G, Roman E, Cordoba J, Torrens M, Poca M, Torras X, Villanueva C, et al. Cognitive dysfunction in cirrhosis is associated with falls: a prospective study. Hepatology. 2012;55:1922–1930. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources