

Can point-of-care urine LAM strip testing for tuberculosis add value to clinical decision making in hospitalised HIV-infected persons?
- PMID: 23390504
- PMCID: PMC3563660
- DOI: 10.1371/journal.pone.0054875
Can point-of-care urine LAM strip testing for tuberculosis add value to clinical decision making in hospitalised HIV-infected persons?
Abstract
Background: The urine lipoarabinomannan (LAM) strip-test (Determine®-TB) can rapidly rule-in TB in HIV-infected persons with advanced immunosuppression. However, given high rates of empiric treatment amongst hospitalised patients in high-burden settings (≈ 50%) it is unclear whether LAM can add any value to clinical decision making, or identify a subset of patients with unfavourable outcomes that would otherwise have been missed by empiric treatment.
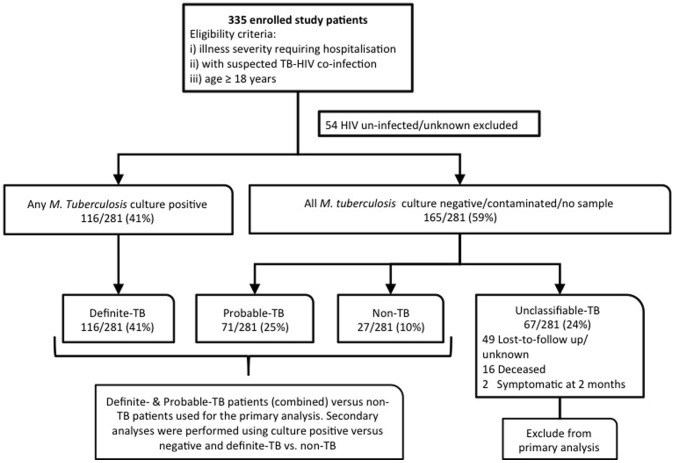
Methods: 281 HIV-infected hospitalised patients with suspected TB received urine LAM strip testing, and were categorised as definite (culture-positive), probable-, or non-TB. Both the proportion and morbidity of TB cases identified by LAM testing, early empiric treatment (initiated prior to test result availability) and a set of clinical predictors were compared across groups.
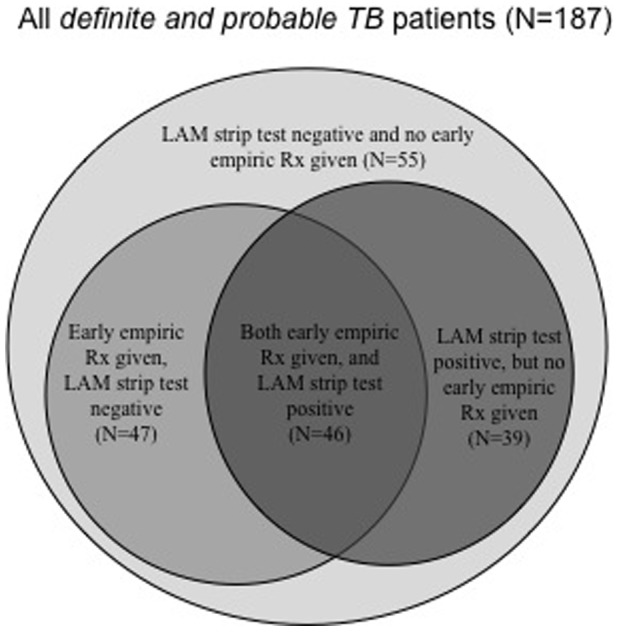
Results: 187/281 patients had either definite- (n = 116) or probable-TB (n = 71). As a rule-in test for definite and probable-TB, LAM identified a similar proportion of TB cases compared to early empiric treatment (85/187 vs. 93/187, p = 0.4), but a greater proportion than classified by a set of clinical predictors alone (19/187; p<0.001). Thirty-nine of the 187 (21%) LAM-positive patients who had either definite- or probable-TB were missed by early empiric treatment, and of these 25/39 (64%) would also have been missed by smear microscopy. Thus, 25/187 (8%) of definite- or probable-TB patients with otherwise delayed initiation of TB treatment could be detected by the LAM strip test. LAM-positive patients missed by early empiric treatment had a lower median CD4 count (p = 0.008), a higher median illness severity score (p = 0.001) and increased urea levels (p = 0.002) compared to LAM-negative patients given early empiric treatment.
Conclusions: LAM strip testing outperformed TB diagnosis based on clinical criteria but in day-to-day practice identified a similar proportion of patients compared to early empiric treatment. However, compared to empiric treatment, LAM identified a different subset of patients with more advanced immunosuppression and greater disease severity.
Conflict of interest statement
Figures
References
-
- Edginton ME, Wong ML, Phofa R, Mahlaba D, Hodkinson HJ (2005) Tuberculosis at Chris Hani Baragwanath Hospital: numbers of patients diagnosed and outcomes of referrals to district clinics. The international journal of tuberculosis and lung disease : the official journal of the International Union against Tuberculosis and Lung Disease 9: 398–402. - PubMed
-
- Theron G, Peter J, Dheda K (2011) Xpert MTB/RIF test for tuberculosis. Lancet 378: 481; author reply 482–483. - PubMed
-
- Theron G, Peter J, van Zyl-Smit R, Mishra H, Streicher E, et al. (2011) Evaluation of the Xpert MTB/RIF assay for the diagnosis of pulmonary tuberculosis in a high HIV prevalence setting. American journal of respiratory and critical care medicine 184: 132–140. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
