

The natural history of multiple system atrophy: a prospective European cohort study
- PMID: 23391524
- PMCID: PMC3581815
- DOI: 10.1016/S1474-4422(12)70327-7
The natural history of multiple system atrophy: a prospective European cohort study
Abstract
Background: Multiple system atrophy (MSA) is a fatal and still poorly understood degenerative movement disorder that is characterised by autonomic failure, cerebellar ataxia, and parkinsonism in various combinations. Here we present the final analysis of a prospective multicentre study by the European MSA Study Group to investigate the natural history of MSA.
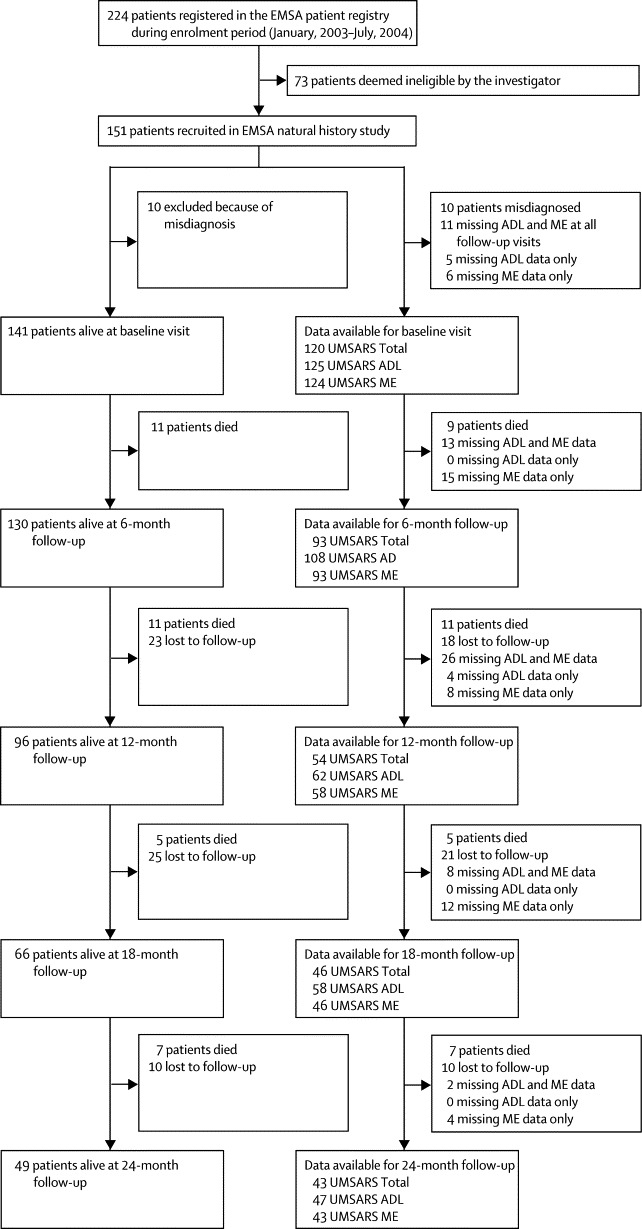
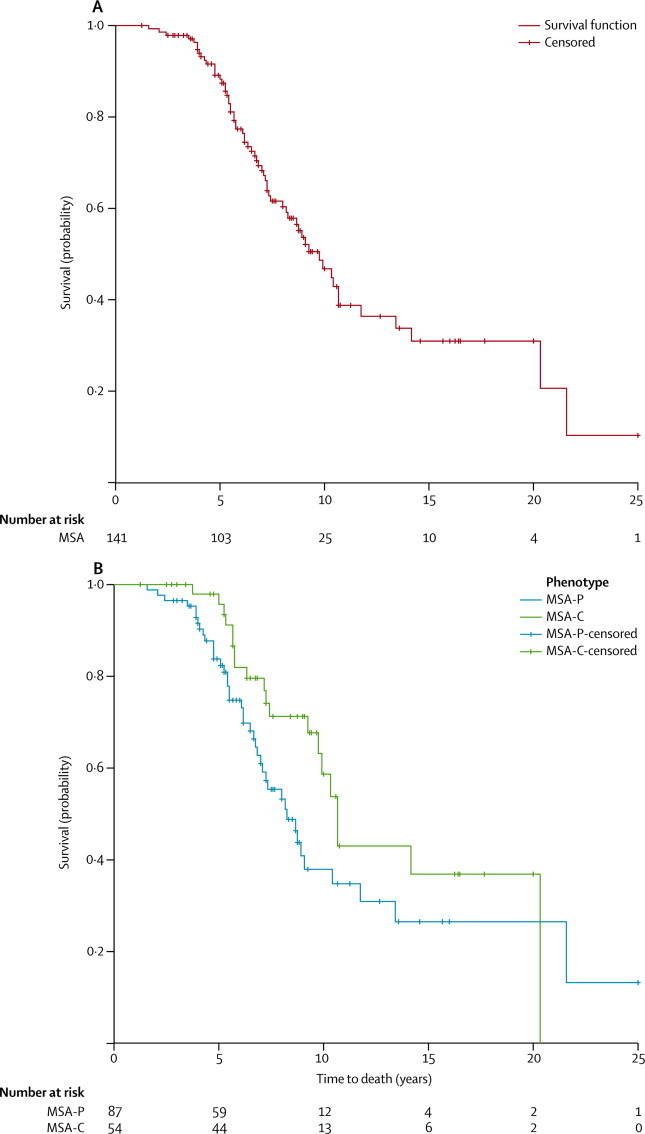
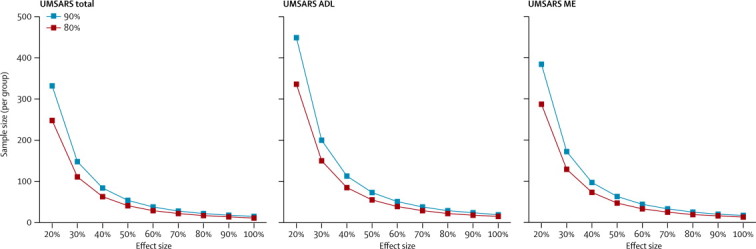
Methods: Patients with a clinical diagnosis of MSA were recruited and followed up clinically for 2 years. Vital status was ascertained 2 years after study completion. Disease progression was assessed using the unified MSA rating scale (UMSARS), a disease-specific questionnaire that enables the semiquantitative rating of autonomic and motor impairment in patients with MSA. Additional rating methods were applied to grade global disease severity, autonomic symptoms, and quality of life. Survival was calculated using a Kaplan-Meier analysis and predictors were identified in a Cox regression model. Group differences were analysed by parametric tests and non-parametric tests as appropriate. Sample size estimates were calculated using a paired two-group t test.
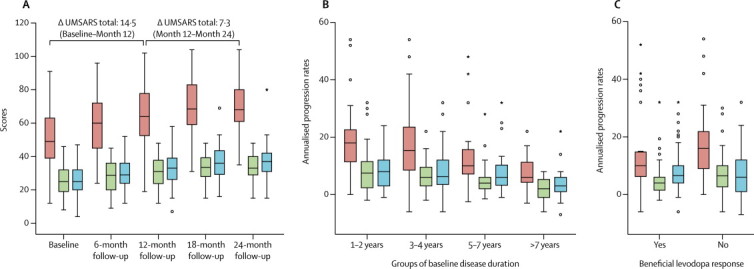
Findings: 141 patients with moderately severe disease fulfilled the consensus criteria for MSA. Mean age at symptom onset was 56·2 (SD 8·4) years. Median survival from symptom onset as determined by Kaplan-Meier analysis was 9·8 years (95% CI 8·1-11·4). The parkinsonian variant of MSA (hazard ratio [HR] 2·08, 95% CI 1·09-3·97; p=0·026) and incomplete bladder emptying (HR 2·10, 1·02-4·30; p=0·044) predicted shorter survival. 24-month progression rates of UMSARS activities of daily living, motor examination, and total scores were 49% (9·4 [SD 5·9]), 74% (12·9 [8·5]), and 57% (21·9 [11·9]), respectively, relative to baseline scores. Autonomic symptom scores progressed throughout the follow-up. Shorter symptom duration at baseline (OR 0·68, 0·5-0·9; p=0·006) and absent levodopa response (OR 3·4, 1·1-10·2; p=0·03) predicted rapid UMSARS progression. Sample size estimation showed that an interventional trial with 258 patients (129 per group) would be able to detect a 30% effect size in 1-year UMSARS motor examination decline rates at 80% power.
Interpretation: Our prospective dataset provides new insights into the evolution of MSA based on a follow-up period that exceeds that of previous studies. It also represents a useful resource for patient counselling and planning of multicentre trials.
Copyright © 2013 Elsevier Ltd. All rights reserved.
Figures
Comment in
-
A milestone on the way to therapy for MSA.Lancet Neurol. 2013 Mar;12(3):222-3. doi: 10.1016/S1474-4422(13)70023-1. Epub 2013 Feb 5. Lancet Neurol. 2013. PMID: 23391525 No abstract available.
-
Assessment of long-term outcome in neurological disease.J Neurol. 2013 Jun;260(6):1693-5. doi: 10.1007/s00415-013-6966-3. J Neurol. 2013. PMID: 23719788 No abstract available.
References
-
- Wenning GK, Colosimo C, Geser F, Poewe W. Multiple system atrophy. Lancet Neurol. 2004;3:93–103. - PubMed
-
- Gilman S, Low PA, Quinn N. Consensus statement on the diagnosis of multiple system atrophy. J Neurol Sci. 1999;163:94–98. - PubMed
-
- Wenning GK, Ben Shlomo Y, Magalhaes M, Daniel SE, Quinn NP. Clinical features and natural history of multiple system atrophy. An analysis of 100 cases. Brain. 1994;117:835–845. - PubMed
-
- Colosimo C. Nonmotor presentations of multiple system atrophy. Nature Rev Neurol. 2011;7:295–298. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
