

Mortality associated with delays between clinic entry and ART initiation in resource-limited settings: results of a transition-state model
- PMID: 23392457
- PMCID: PMC3647455
- DOI: 10.1097/QAI.0b013e3182893fb4
Mortality associated with delays between clinic entry and ART initiation in resource-limited settings: results of a transition-state model
Abstract
Objective: To estimate the mortality impact of delay in antiretroviral therapy (ART) initiation from the time of entry into care.
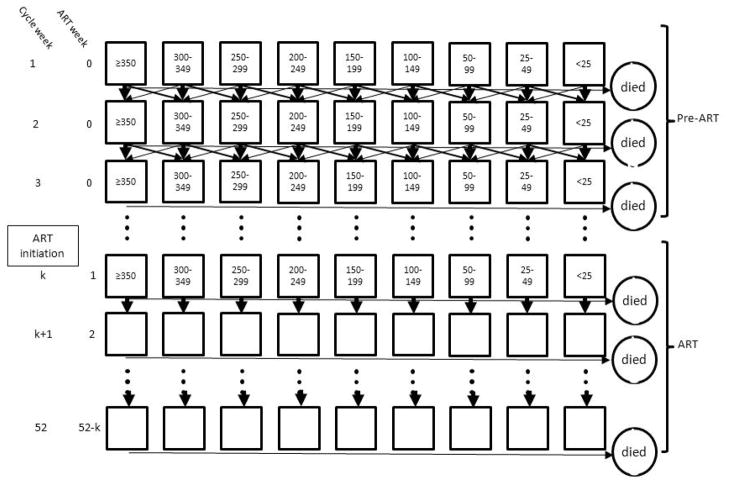
Design: A state-transition Markov process model. This technique allows for assessing mortality before and after ART initiation associated with delays in ART initiation among a general population of ART-eligible patients without conducting a randomized trial.
Methods: We used patient-level data from 3 South African cohorts to determine transition probabilities for pre-ART CD4 count changes and pre-ART and on-ART mortality. For each parameter, we generated probabilities and distributions for Monte Carlo simulations with 1-week cycles to estimate mortality 52 weeks from clinic entry.
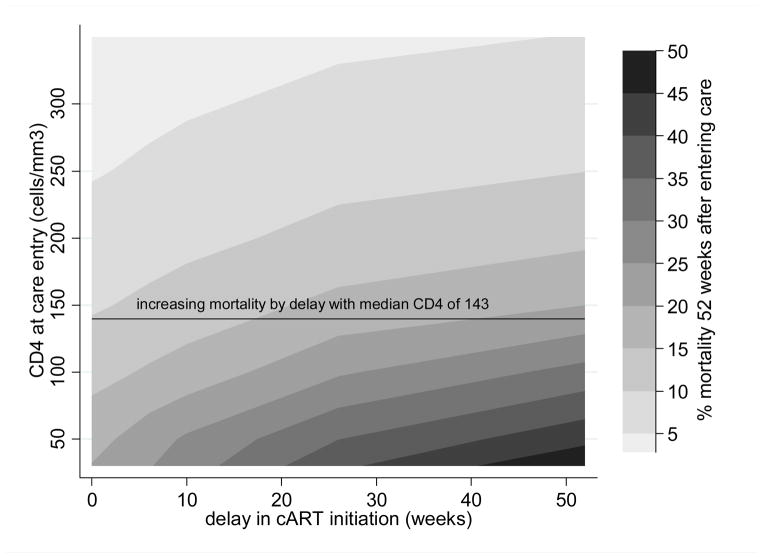
Results: We estimated an increase in mortality from 11.0% to 14.7% (relative increase of 34%) with a 10-week delay in ART for patients entering care with our pre-ART cohort CD4 distribution. When we examined low CD4 ranges, the relative increase in mortality delays remained similar; however, the absolute increase in mortality rose. For example, among patients entering with CD4 count 50-99 cells per cubic millimeter, 12-month mortality increased from 13.3% with no delay compared with 17.0% with a 10-week delay and 22.9% with a 6-month delay.
Conclusions: Delays in ART initiation, common in routine HIV programs, can lead to important increases in mortality. Prompt ART initiation for patients entering clinical care and eligible for ART, especially those with lower CD4 counts, could be a relatively low-cost approach with a potential marked impact on mortality.
Conflict of interest statement
Conflicts of interest: All authors, no conflicts
Figures
References
-
- Lohse N, Hansen AB, Pedersen G, Kronborg G, Gerstoft J, Sorensen HT, Vaeth M, Obel N. Survival of persons with and without HIV infection in Denmark, 1995–2005. Ann Intern Med. 2007;146:87–95. - PubMed
-
- Hogg RS, Heath KV, Yip B, Craib KJ, O’Shaughnessy MV, Schechter MT, Montaner JS. Improved survival among HIV-infected individuals following initiation of antiretroviral therapy. JAMA. 1998;279:450–454. - PubMed
-
- El-Sadr W, Neaton J The SMART Study Investigators. Episodic CD4-guided use of antiretroviral therapy is inferior to continuous therapy: results of the SMART study. Program and abstracts of the 13th Conference on Retroviruses and Opportunistic Infections; 2006.
-
- Kitahata MM, Gange SJ, Abraham AG, Merriman B, Saag MS, Justice AC, Hogg RS, Deeks SG, Eron JJ, Brooks JT, Rourke SB, Gill MJ, Bosch RJ, Martin JN, Klein MB, Jacobson LP, Rodriguez B, Sterling TR, Kirk GD, Napravnik S, Rachlis AR, Calzavara LM, Horberg MA, Silverberg MJ, Gebo KA, Goedert JJ, Benson CA, Collier AC, Van Rompaey SE, Crane HM, McKaig RG, Lau B, Freeman AM, Moore RD. Effect of early versus deferred antiretroviral therapy for HIV on survival. N Engl J Med. 2009;360:1815–26. - PMC - PubMed
-
- Sterne JA, May M, Costagliola D, de WF, Phillips AN, Harris R, Funk MJ, Geskus RB, Gill J, Dabis F, Miro JM, Justice AC, Ledergerber B, Fatkenheuer G, Hogg RS, Monforte AD, Saag M, Smith C, Staszewski S, Egger M, Cole SR. Timing of initiation of antiretroviral therapy in AIDS-free HIV-1-infected patients: a collaborative analysis of 18 HIV cohort studies. Lancet. 2009;373:1352–63. - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
