

Dexamethasone mimics aspects of physiological acclimatization to 8 hours of hypoxia but suppresses plasma erythropoietin
- PMID: 23393065
- PMCID: PMC3633439
- DOI: 10.1152/japplphysiol.01414.2012
Dexamethasone mimics aspects of physiological acclimatization to 8 hours of hypoxia but suppresses plasma erythropoietin
Abstract
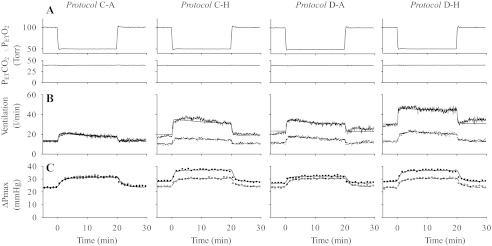
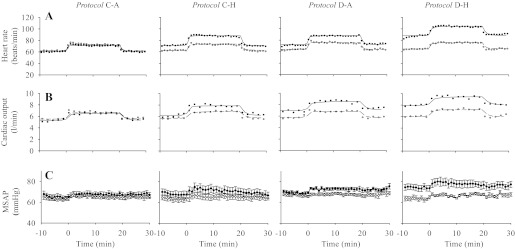
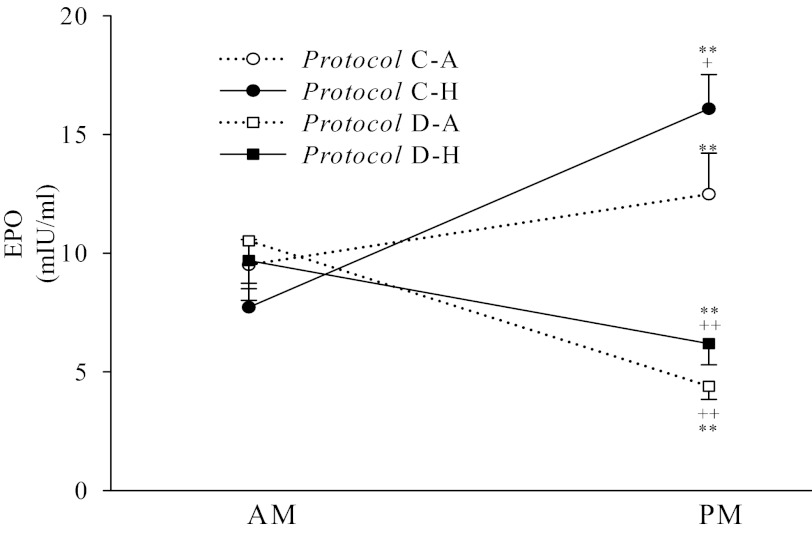
Dexamethasone ameliorates the severity of acute mountain sickness (AMS) but it is unknown whether it obtunds normal physiological responses to hypoxia. We studied whether dexamethasone enhanced or inhibited the ventilatory, cardiovascular, and pulmonary vascular responses to sustained (8 h) hypoxia. Eight healthy volunteers were studied, each on four separate occasions, permitting four different protocols. These were: dexamethasone (20 mg orally) beginning 2 h before a control period of 8 h of air breathing; dexamethasone with 8 h of isocapnic hypoxia (end-tidal Po(2) = 50 Torr); placebo with 8 h of air breathing; and placebo with 8 h of isocapnic hypoxia. Before and after each protocol, the following were determined under both euoxic and hypoxic conditions: ventilation; pulmonary artery pressure (estimated using echocardiography to assess maximum tricuspid pressure difference); heart rate; and cardiac output. Plasma concentrations of erythropoietin (EPO) were also determined. Dexamethasone had no early (2-h) effect on any variable. Both dexamethasone and 8 h of hypoxia increased euoxic values of ventilation, pulmonary artery pressure, and heart rate, together with the ventilatory sensitivity to acute hypoxia. These effects were independent and additive. Eight hours of hypoxia, but not dexamethasone, increased the sensitivity of pulmonary artery pressure to acute hypoxia. Dexamethasone, but not 8 h of hypoxia, increased both cardiac output and systemic arterial pressure. Dexamethasone abolished the rise in EPO induced by 8 h of hypoxia. In summary, dexamethasone enhances ventilatory acclimatization to hypoxia. Thus, dexamethasone in AMS may improve oxygenation and thereby indirectly lower pulmonary artery pressure.
Figures
References
-
- Balanos GM, Talbot NP, Dorrington KL, Robbins PA. Human pulmonary vascular response to 4 h of hypercapnia and hypocapnia measured using Doppler echocardiography. J Appl Physiol 94: 1543–1551, 2003 - PubMed
-
- Balanos GM, Talbot NP, Robbins PA, Dorrington KL. Separating the direct effect of hypoxia from the indirect effect of changes in cardiac output on the maximum pressure difference across the tricuspid valve in healthy humans. Pflugers Arch 450: 372–380, 2005 - PubMed
-
- Bernhard WN, Schalick LM, Gittelsohn A. Dexamethasone for prophylaxis against acute mountain sickness during rapid ascent to 5334 m. J Wilderness Med 5: 331–338, 1994
-
- Bushuev VI, Miasnikova GY, Sergueeva AI, Polyakova LA, Okhotin D, Debebe Z, Nekhai S, Castro OL, Prchal JT, Gordeuk VR. Endothelin-1, vascular endothelial growth factor and systolic pulmonary artery pressure in patients with Chuvash polycythemia. Haematologica 91: 744–749, 2006 - PubMed
-
- Clar C, Dorrington KL, Fatemian M, Robbins PA. Effects of 8 h of isocapnic hypoxia with and without muscarinic blockade on ventilation and heart rate in humans. Exp Physiol 86: 529–538, 2001 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials