

Predictors of mortality and long-term outcomes in treated Cushing's disease: a study of 346 patients
- PMID: 23393167
- PMCID: PMC3590483
- DOI: 10.1210/jc.2012-2893
Predictors of mortality and long-term outcomes in treated Cushing's disease: a study of 346 patients
Abstract
Context: Active Cushing's disease (CD) confers a 4-fold increase in mortality and is associated with significant morbidities. Although excess mortality risk may persist even after CD treatment, predictors of risk in treated CD are not well understood.
Objective: To identify predictors of mortality, cardiovascular (CV) disease, and recurrence after long-term follow-up among patients with treated CD.
Design, setting, and patients: A retrospective chart review was conducted to evaluate patients with CD who underwent transsphenoidal adenectomy with a single surgeon.
Outcome measures: Patients were categorized based on disease response after initial treatment. Cox proportional hazard models identified predictors of mortality, recurrence, and CV outcomes in the overall cohort and each subgroup.
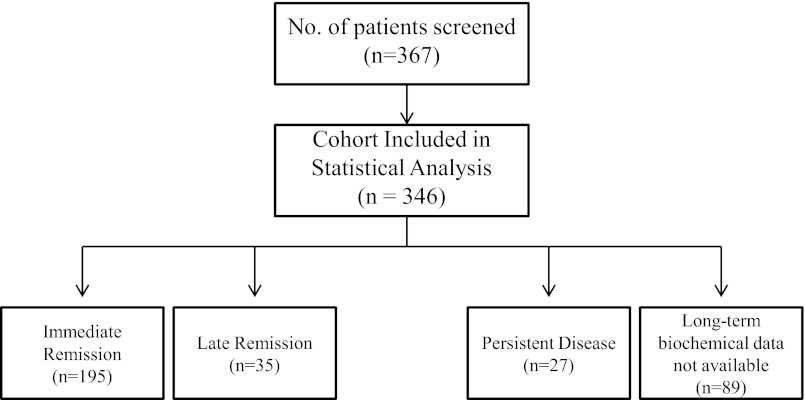
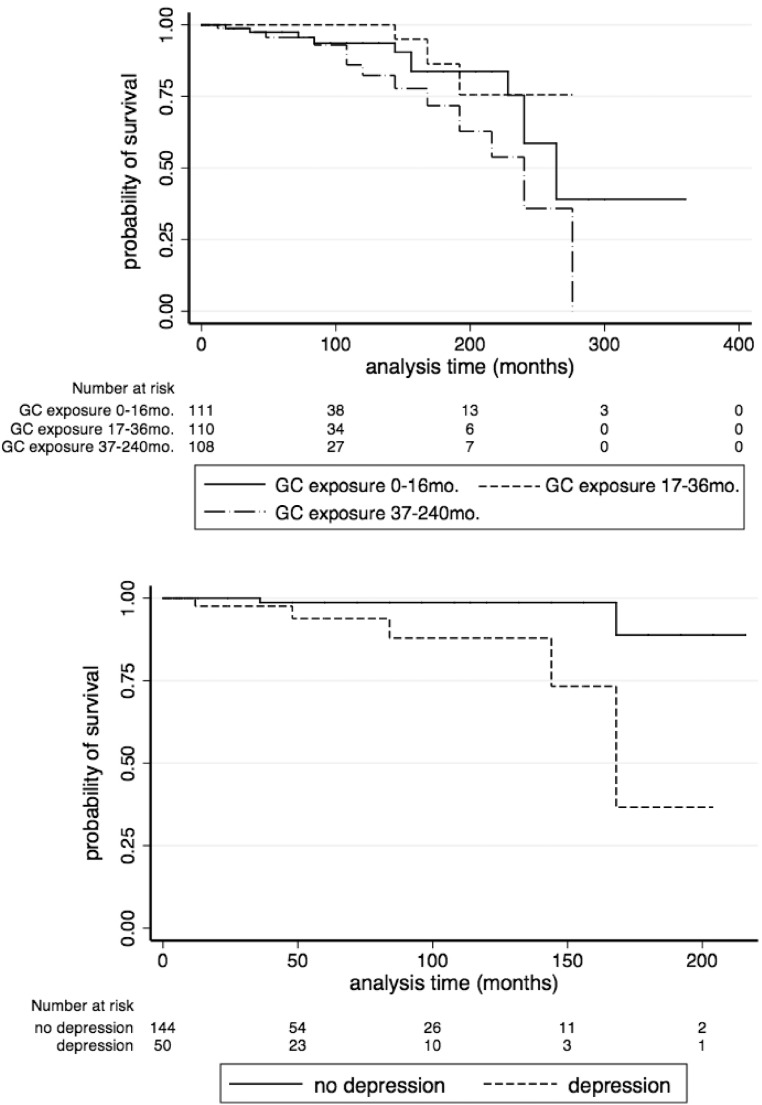
Results: Three hundred forty-six subjects were included. Mean age was 39.9 years, and mean duration of follow-up was 6.3 years (range, 1 mo to 30 y). Duration of exposure to excess glucocorticoids, estimated by duration of symptoms before diagnosis until remission was achieved by any means, was 40.0 months. Multivariate analyses demonstrated that duration of glucocorticoid exposure elevated the risk of death (P = .038), as did older age at diagnosis (P = 0.0001) and preoperative ACTH concentration (P = .007). Among patients who achieved remission, depression increased the hazard of death (P < .01). Male sex, age at diagnosis, diabetes, and depression elevated the risk of CV disease (P < .05).
Conclusion: Long-term follow-up of a large cohort of treated patients with CD identified several novel predictors of mortality. These data illustrate the importance of early recognition and treatment of CD. Long-term follow-up, with management of persistent comorbidities, is needed even after successful treatment of CD.
Figures
References
-
- Etxabe J, Vazquez JA. Morbidity and mortality in Cushing's disease: an epidemiological approach. Clin Endocrinol (Oxf). 1994;40:479–484 - PubMed
-
- Lindholm J, Juul S, Jørgensen JO, et al. Incidence and late prognosis of cushing's syndrome: a population-based study. J Clin Endocrinol Metab. 2001;86:117–123 - PubMed
-
- Cushing H. The basophil adenomas of the pituitary body and their clinical manifestations (pituitary basophilism). 1932. Obes Res. 1994;2:486–508 - PubMed
-
- Plotz CM, Knowlton AI, Ragan C. The natural history of Cushing's syndrome. Am J Med. 1952;13:597–614 - PubMed
-
- Pivonello R, Faggiano A, Lombardi G, Colao A. The metabolic syndrome and cardiovascular risk in Cushing's syndrome. Endocrinol Metab Clin North Am. 2005;34:327–339 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
