

Causal relationship between obesity and vitamin D status: bi-directional Mendelian randomization analysis of multiple cohorts
- PMID: 23393431
- PMCID: PMC3564800
- DOI: 10.1371/journal.pmed.1001383
Causal relationship between obesity and vitamin D status: bi-directional Mendelian randomization analysis of multiple cohorts
Abstract
Background: Obesity is associated with vitamin D deficiency, and both are areas of active public health concern. We explored the causality and direction of the relationship between body mass index (BMI) and 25-hydroxyvitamin D [25(OH)D] using genetic markers as instrumental variables (IVs) in bi-directional Mendelian randomization (MR) analysis.
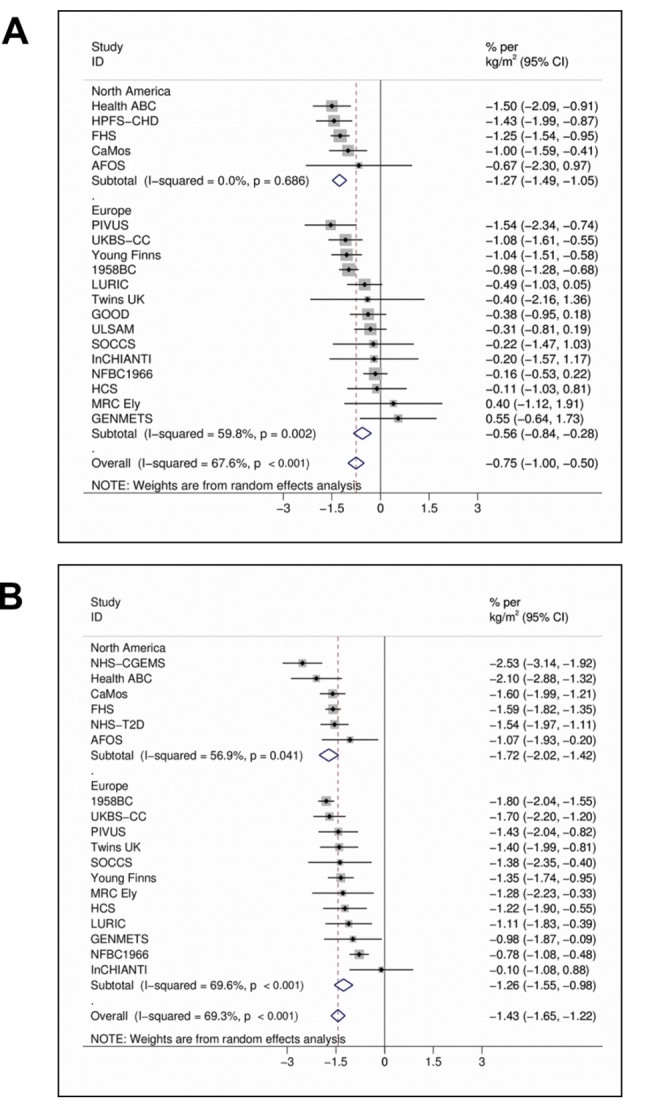
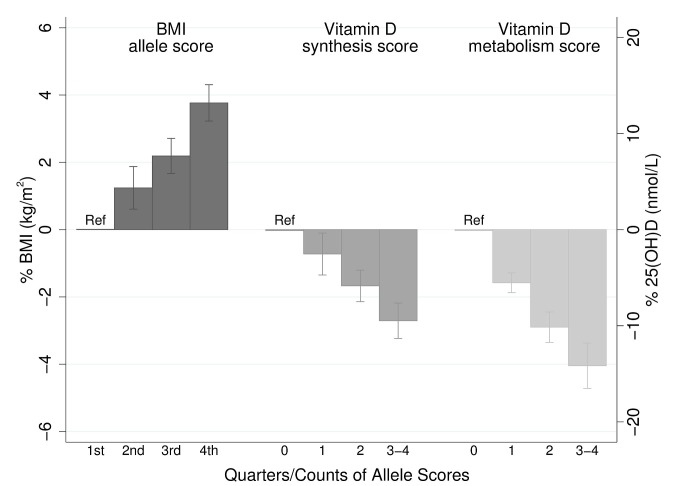
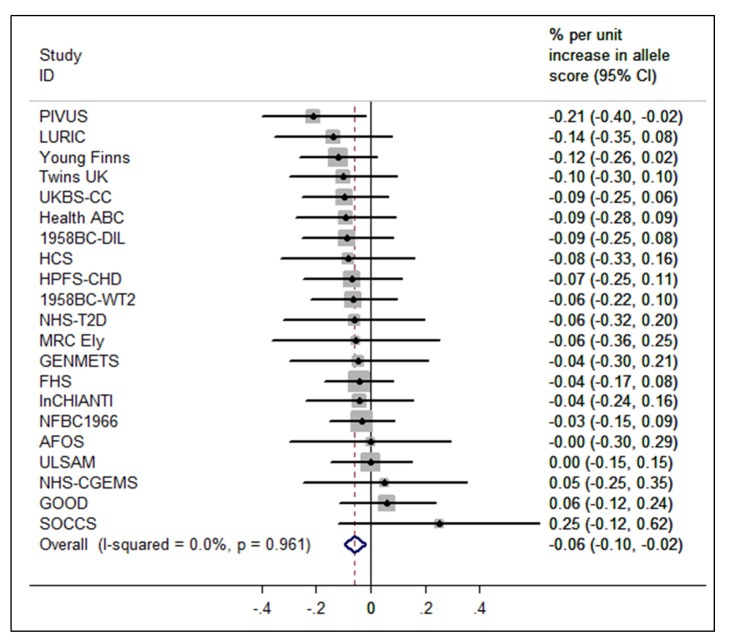
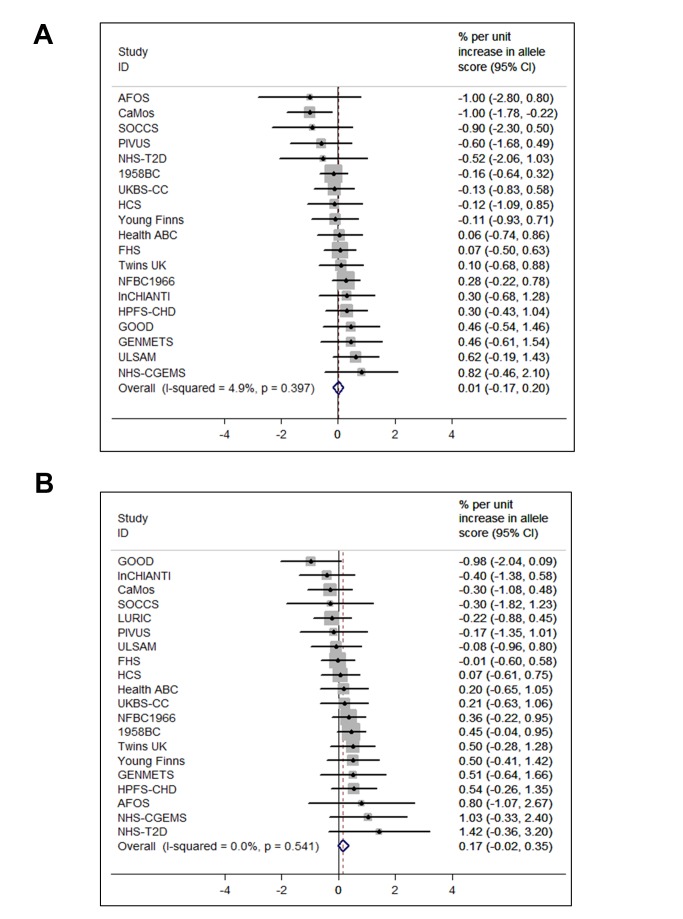
Methods and findings: We used information from 21 adult cohorts (up to 42,024 participants) with 12 BMI-related SNPs (combined in an allelic score) to produce an instrument for BMI and four SNPs associated with 25(OH)D (combined in two allelic scores, separately for genes encoding its synthesis or metabolism) as an instrument for vitamin D. Regression estimates for the IVs (allele scores) were generated within-study and pooled by meta-analysis to generate summary effects. Associations between vitamin D scores and BMI were confirmed in the Genetic Investigation of Anthropometric Traits (GIANT) consortium (n = 123,864). Each 1 kg/m(2) higher BMI was associated with 1.15% lower 25(OH)D (p = 6.52×10⁻²⁷). The BMI allele score was associated both with BMI (p = 6.30×10⁻⁶²) and 25(OH)D (-0.06% [95% CI -0.10 to -0.02], p = 0.004) in the cohorts that underwent meta-analysis. The two vitamin D allele scores were strongly associated with 25(OH)D (p≤8.07×10⁻⁵⁷ for both scores) but not with BMI (synthesis score, p = 0.88; metabolism score, p = 0.08) in the meta-analysis. A 10% higher genetically instrumented BMI was associated with 4.2% lower 25(OH)D concentrations (IV ratio: -4.2 [95% CI -7.1 to -1.3], p = 0.005). No association was seen for genetically instrumented 25(OH)D with BMI, a finding that was confirmed using data from the GIANT consortium (p≥0.57 for both vitamin D scores).
Conclusions: On the basis of a bi-directional genetic approach that limits confounding, our study suggests that a higher BMI leads to lower 25(OH)D, while any effects of lower 25(OH)D increasing BMI are likely to be small. Population level interventions to reduce BMI are expected to decrease the prevalence of vitamin D deficiency.
Conflict of interest statement
LTH is currently supported by a Canada Institute of Research (CIHR) Fellowship award. CC has received honoraria and consulting fees from Amgen, Eli Lilly, Medtronic, Merck, Novartis, and Servier. WM is an employee of synlab laboratory services GmbH. Synlab offers vitamin D testing. TJW is on the scientific advisory board for Diasorin Inc. and has received research support from them. JCW is 90% employed by GlaxoSmithKline (GSK) whilst maintaining a 10% appointment at London School of Hygiene & Tropical Medicine (LSHTM), and holds GSK shares. All other authors declare that no competing interests exist.
Figures
References
-
- Baskin ML, Ard J, Franklin F, Allison DB (2005) Prevalence of obesity in the United States. Obes Rev 6: 5–7. - PubMed
-
- Ogden CL, Carroll MD, Curtin LR, Lamb MM, Flegal KM (2010) Prevalence of high body mass index in US children and adolescents, 2007–2008. JAMA 303: 242–249. - PubMed
-
- Flegal KM, Carroll MD, Kit BK, Ogden CL (2012) Prevalence of obesity and trends in the distribution of body mass index among US adults, 1999–2010. JAMA 307: 491–497. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- G0801056/MRC_/Medical Research Council/United Kingdom
- CZH/4/529/CSO_/Chief Scientist Office/United Kingdom
- U.1475.00.003.00010.02(74238)/MRC_/Medical Research Council/United Kingdom
- 13147/ARC_/Arthritis Research UK/United Kingdom
- DH_/Department of Health/United Kingdom
- MC_U106179471/MRC_/Medical Research Council/United Kingdom
- U.1475.00.003.00010.02(74242)/MRC_/Medical Research Council/United Kingdom
- 14136/CRUK_/Cancer Research UK/United Kingdom
- 13085/ARC_/Arthritis Research UK/United Kingdom
- FS05/125/BHF_/British Heart Foundation/United Kingdom
- 13230/ARC_/Arthritis Research UK/United Kingdom
- MC_U147574233/MRC_/Medical Research Council/United Kingdom
- 17265/ARC_/Arthritis Research UK/United Kingdom
- G0601653/MRC_/Medical Research Council/United Kingdom
- K05 AA017688/AA/NIAAA NIH HHS/United States
- U.1475.00.002.00001.01(74218)/MRC_/Medical Research Council/United Kingdom
- 16349/ARC_/Arthritis Research UK/United Kingdom
- MC_U147585827/MRC_/Medical Research Council/United Kingdom
- 13181/ARC_/Arthritis Research UK/United Kingdom
- 12076/CRUK_/Cancer Research UK/United Kingdom
- PG/09/023/BHF_/British Heart Foundation/United Kingdom
- K01 AG030506/AG/NIA NIH HHS/United States
- MC_U147585819/MRC_/Medical Research Council/United Kingdom
- G1000143/MRC_/Medical Research Council/United Kingdom
- MC_U147574215/MRC_/Medical Research Council/United Kingdom
- 17413/ARC_/Arthritis Research UK/United Kingdom
- 13157/ARC_/Arthritis Research UK/United Kingdom
- MC_U127527198/MRC_/Medical Research Council/United Kingdom
- MC_UP_A620_1014/MRC_/Medical Research Council/United Kingdom
- MC_U147574236/MRC_/Medical Research Council/United Kingdom
- G0401527/MRC_/Medical Research Council/United Kingdom
- 090532/WT_/Wellcome Trust/United Kingdom
- MC_PC_U127561128/MRC_/Medical Research Council/United Kingdom
- PG/09/023/26806/BHF_/British Heart Foundation/United Kingdom
- MC_U106188470/MRC_/Medical Research Council/United Kingdom
- 16095/ARC_/Arthritis Research UK/United Kingdom
- G0400491/MRC_/Medical Research Council/United Kingdom
- MC_U147574217/MRC_/Medical Research Council/United Kingdom
- MC_U147585824/MRC_/Medical Research Council/United Kingdom
- MC_U147574221/MRC_/Medical Research Council/United Kingdom
- P30 AG021332/AG/NIA NIH HHS/United States
- U.1475.00.003.00010.02(74237)/MRC_/Medical Research Council/United Kingdom
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
