

A trial of imaging selection and endovascular treatment for ischemic stroke
- PMID: 23394476
- PMCID: PMC3690785
- DOI: 10.1056/NEJMoa1212793
A trial of imaging selection and endovascular treatment for ischemic stroke
Abstract
Background: Whether brain imaging can identify patients who are most likely to benefit from therapies for acute ischemic stroke and whether endovascular thrombectomy improves clinical outcomes in such patients remains unclear.
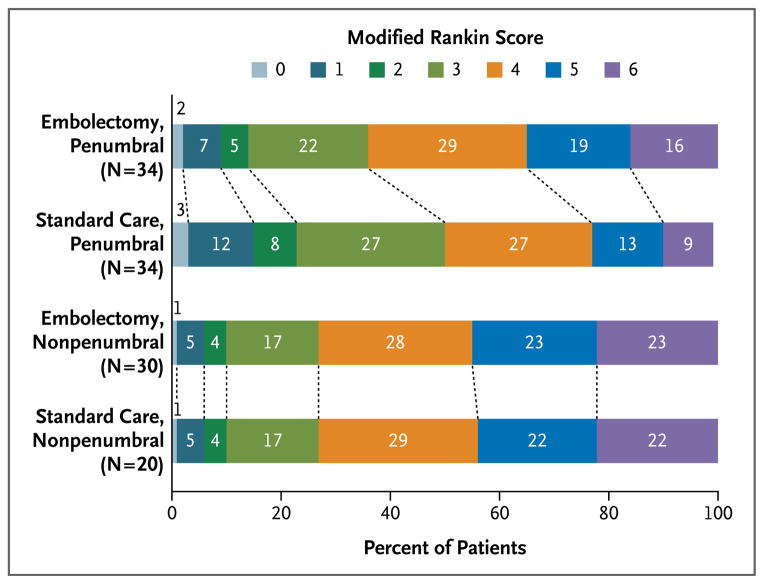
Methods: In this study, we randomly assigned patients within 8 hours after the onset of large-vessel, anterior-circulation strokes to undergo mechanical embolectomy (Merci Retriever or Penumbra System) or receive standard care. All patients underwent pretreatment computed tomography or magnetic resonance imaging of the brain. Randomization was stratified according to whether the patient had a favorable penumbral pattern (substantial salvageable tissue and small infarct core) or a nonpenumbral pattern (large core or small or absent penumbra). We assessed outcomes using the 90-day modified Rankin scale, ranging from 0 (no symptoms) to 6 (dead).
Results: Among 118 eligible patients, the mean age was 65.5 years, the mean time to enrollment was 5.5 hours, and 58% had a favorable penumbral pattern. Revascularization in the embolectomy group was achieved in 67% of the patients. Ninety-day mortality was 21%, and the rate of symptomatic intracranial hemorrhage was 4%; neither rate differed across groups. Among all patients, mean scores on the modified Rankin scale did not differ between embolectomy and standard care (3.9 vs. 3.9, P=0.99). Embolectomy was not superior to standard care in patients with either a favorable penumbral pattern (mean score, 3.9 vs. 3.4; P=0.23) or a nonpenumbral pattern (mean score, 4.0 vs. 4.4; P=0.32). In the primary analysis of scores on the 90-day modified Rankin scale, there was no interaction between the pretreatment imaging pattern and treatment assignment (P=0.14).
Conclusions: A favorable penumbral pattern on neuroimaging did not identify patients who would differentially benefit from endovascular therapy for acute ischemic stroke, nor was embolectomy shown to be superior to standard care. (Funded by the National Institute of Neurological Disorders and Stroke; MR RESCUE ClinicalTrials.gov number, NCT00389467.).
Figures

Comment in
-
Endovascular treatment for acute ischemic stroke--still unproven.N Engl J Med. 2013 Mar 7;368(10):952-5. doi: 10.1056/NEJMe1215730. Epub 2013 Feb 8. N Engl J Med. 2013. PMID: 23394477 No abstract available.
-
[Is invasive therapy for stroke better than lysis? - time periods during stroke treatment have to be shortened].Dtsch Med Wochenschr. 2013 Apr;138(17):874-5. doi: 10.1055/s-0032-1329045. Epub 2013 Apr 16. Dtsch Med Wochenschr. 2013. PMID: 23592341 German. No abstract available.
-
Commentary: Societal statement on recent acute stroke intervention trials: results and implications.Neurosurgery. 2013 Aug;73(2):E375-9. doi: 10.1227/01.neu.0000430514.46473.4f. Neurosurgery. 2013. PMID: 23632768 No abstract available.
-
Endovascular treatment for acute ischemic stroke.N Engl J Med. 2013 Jun 20;368(25):2430. doi: 10.1056/NEJMc1304759. N Engl J Med. 2013. PMID: 23782183 No abstract available.
-
Endovascular treatment for acute ischemic stroke.N Engl J Med. 2013 Jun 20;368(25):2430-1. doi: 10.1056/NEJMc1304759. N Engl J Med. 2013. PMID: 23782184 No abstract available.
-
Endovascular treatment for acute ischemic stroke.N Engl J Med. 2013 Jun 20;368(25):2431. doi: 10.1056/NEJMc1304759. N Engl J Med. 2013. PMID: 23782185 No abstract available.
-
Endovascular treatment for acute ischemic stroke.N Engl J Med. 2013 Jun 20;368(25):2431-2. doi: 10.1056/NEJMc1304759. N Engl J Med. 2013. PMID: 23782186 No abstract available.
-
Endovascular treatment for acute ischemic stroke.N Engl J Med. 2013 Jun 20;368(25):2434-5. doi: 10.1056/NEJMc1304759. N Engl J Med. 2013. PMID: 23802241 No abstract available.
References
-
- The National Institute of Neurological Disorders and Stroke rt-PA Stroke Study Group. . Tissue plasminogen activator for acute ischemic stroke. N Engl J Med. 1995;333:1581–7. - PubMed
-
- Hacke W, Kaste M, Bluhmki E, et al. Thrombolysis with alteplase 3 to 4. 5 hours after acute ischemic stroke. N Engl J Med. 2008;359:1317–29. - PubMed
-
- Fisher M. Characterizing the target of acute stroke therapy. Stroke. 1997;28:866–72. - PubMed
-
- Barber PA, Darby DG, Desmond PM, et al. Prediction of stroke outcome with echoplanar perfusion- and diffusion-weighted MRI. Neurology. 1998;51:418–26. - PubMed
-
- Smith WS, Sung G, Starkman S, et al. Safety and efficacy of mechanical embolectomy in acute ischemic stroke: results of the MERCI trial. Stroke. 2005;36:1432–8. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical