

Frailty in elderly people
- PMID: 23395245
- PMCID: PMC4098658
- DOI: 10.1016/S0140-6736(12)62167-9
Frailty in elderly people
Erratum in
- Lancet. 2013 Oct 19;382(9901):1328
Abstract
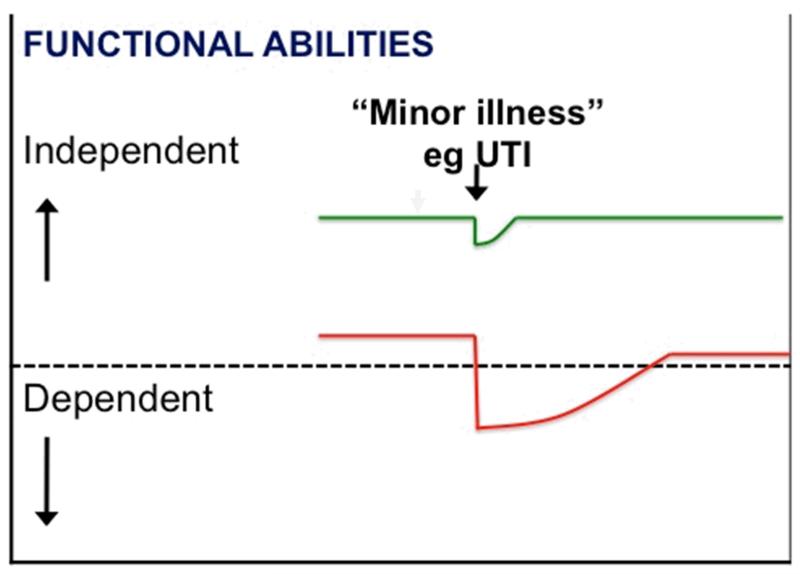
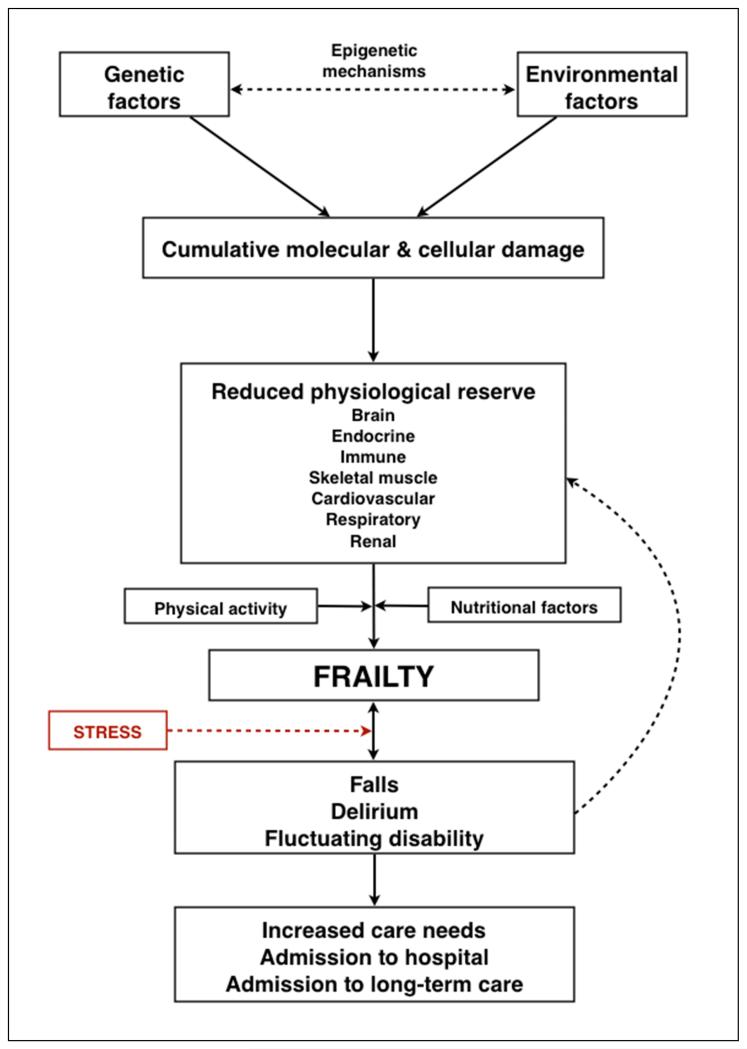
Frailty is the most problematic expression of population ageing. It is a state of vulnerability to poor resolution of homoeostasis after a stressor event and is a consequence of cumulative decline in many physiological systems during a lifetime. This cumulative decline depletes homoeostatic reserves until minor stressor events trigger disproportionate changes in health status. In landmark studies, investigators have developed valid models of frailty and these models have allowed epidemiological investigations that show the association between frailty and adverse health outcomes. We need to develop more efficient methods to detect frailty and measure its severity in routine clinical practice, especially methods that are useful for primary care. Such progress would greatly inform the appropriate selection of elderly people for invasive procedures or drug treatments and would be the basis for a shift in the care of frail elderly people towards more appropriate goal-directed care.
Copyright © 2013 Elsevier Ltd. All rights reserved.
Figures
References
-
- Kinsella K, Phillips D. Global Aging: The Challenge of Success. Population Reference Bureau; Washington, DC: 2005. ( Population Bulletin 60, no.1 ).
-
- The World at Six Billion . Population Division. Department of Economic and Social Affairs. United Nations Secretariat; Oct 12, 1999. Available at www.un.org/esa/population/publications/sixbillion/sixbilpart1.pdf.
-
- Fried LP, Tangen CM, Walston J, Newman AB, Hirsch C, Gottdiener J, Seeman T, Tracy R, Kop WJ, Burke G, McBurnie MA. Frailty in older adults: evidence for a phenotype. J Gerontol A Biol Sci Med Sci. 2001;56(3):M146–56. - PubMed
-
- Song X, Mitnitski A, Rockwood K. Prevalence and 10-year outcomes of frailty in older adults in relation to deficit accumulation. J Am Geriatr Soc. 2010;58(4):681–7. - PubMed
-
- Walston J, Hadley EC, Ferrucci L, Guralnik JM, Newman AB, Studenski SA, Ershler WB, Harris T, Fried LP. Research agenda for frailty in older adults: toward a better understanding of physiology and etiology: summary from the American Geriatrics Society/National Institute on Aging Research Conference on Frailty in Older Adults. J Am Geriatr Soc. 2006;54(6):991–1001. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
