

US guided corticosteroid injection into the subacromial-subdeltoid bursa: Technique and approach
- PMID: 23396761
- PMCID: PMC3558064
- DOI: 10.1016/j.jus.2011.12.003
US guided corticosteroid injection into the subacromial-subdeltoid bursa: Technique and approach
Abstract
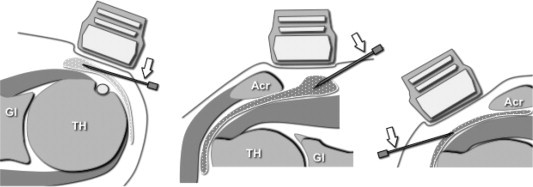
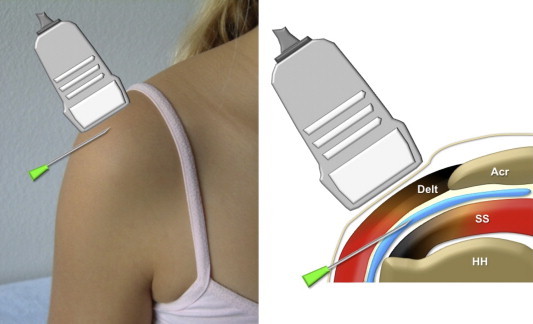
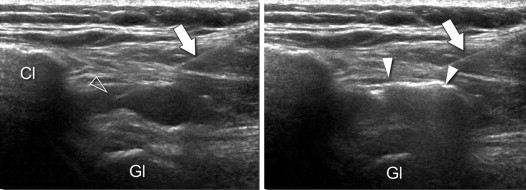
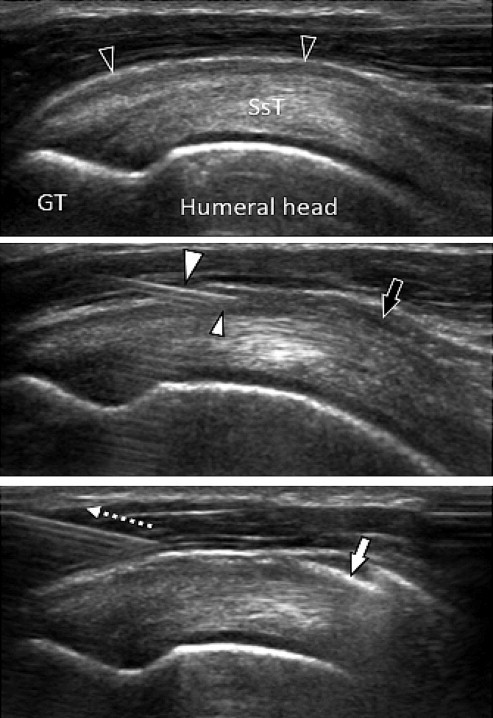
Local injection of cortisone derivatives, sometimes combined with local anesthetics, is frequently administered in rheumatology as the treatment of choice in para-articular diseases or as an adjuvant to systemic therapy in the treatment of arthritis.One of the most frequent local corticosteroid injections administered in daily clinical practice by rheumatologists, orthopedic surgeons, physiatrists, sports medicine doctors and general practitioners is injection into the subacromialsubdeltoid bursa in the treatment of bursitis and anterior superior impingement syndrome of the shoulder.Before local corticosteroid injection is administered, it is important to identify possible contraindications and to examine the documentation provided by the patient. Absolute contraindications or those related to the procedure should be evaluated by the prescribing physician but also the physician performing the corticosteroid injection should evaluate possible contraindications to make sure that corticosteroid injection is feasible. The present paper describes the ultrasound (US) guided local corticosteroid injection procedure with particular attention to the equipment required, the position of the patient and the examiner as well as the approach. The main advantage of US guidance during corticosteroid injection is the possibility to identify vascular structures, nerves and tendons situated in the needle path in order to avoid these structures and be sure to inject the drug into the appropriate location. When all rules are complied with and the corticosteroid injection is carried out by an experienced physician, it is virtually painless and is performed in just a few minutes.
SommarioL’infiltrazione locale di derivati cortisonici, uniti o non ad anestetici locali, è una modalità terapeutica di utilizzo molto frequente in reumatologia, praticata come terapia di elezione delle patologie para-articolari o come adiuvante al trattamento sistemico nella cura delle artriti.Una delle più frequenti infiltrazioni locali, nella pratica clinica giornaliera di reumatologi, ortopedici, fisiatri, medici dello sport e medici generici è l’iniezione nella borsa sinoviale sottoacromiondeltoidea, quale trattamento della borsite e nella sindrome da conflitto antero-superiore della spalla.Prima di eseguire una procedura di infiltrazione locale è importante individuare eventuali controindicazioni e visionare la documentazione fornita dal paziente. Anche se la valutazione delle controindicazioni assolute o relative alla procedura spetta, di principio, al medico prescrittore, è compito del medico ecografista che pratica l’infiltrazione accertarsi della fattibilità della infiltrazione e della presenza di eventuali controindicazioni.Viene presentata la tecnica di esecuzione dell’infiltrazione locale ecoguidata, con particolare attenzione al materiale necessario, alla posizione del paziente e dell’esaminatore e alle vie di accesso.I principali vantaggi dell’infiltrazione ecoguidata sono quelli di riconoscere strutture vascolari, nervose e tendinee poste sul decorso dell’ago, in modo da poterle evitare e di poter iniettare il farmaco con certezza nella sede desiderata.Quando tutte le regole vengono rispettate e l’infiltrazione è praticata da un professionista qualificato, è praticamente indolore e viene realizzata in soli pochi minuti.
Keywords: Local corticosteroid injection; Sonography; Subacromial-subdeltoid bursa.
Figures
References
-
- Weidner S., Kellner W., Kellner H. Interventional radiology and the musculoskeletal system. Best Pract Res Clin Rheumatol. 2004;18:945–956. - PubMed
-
- Sibbitt W.L., Jr., Peisajovich A., Michael A.A., Park K.S., Sibbitt R.R., Band P.A. Does sonographic needle guidance affect the clinical outcome of intraarticular injections? J Rheumatol. 2009;36:1892–1902. - PubMed
-
- Jeyapalan K., Choudhary S. Ultrasound-guided injection of triamcinolone and bupivacaine in the management of De Quervain’s disease. Skeletal Radiol. 2009;38:1099–1103. - PubMed
-
- Grassi W., Farina A., Filippucci E., Cervini C. Sonographically guided procedures in rheumatology. Semin Arthritis Rheum. 2001;30:347–353. - PubMed
-
- Jacob D., Cyteval C., Moinard M. L’échographie interventionnelle. J Radiol. 2005;86:1911–1923. - PubMed
LinkOut - more resources
Full Text Sources