

Carpal tunnel: Normal anatomy, anatomical variants and ultrasound technique
- PMID: 23396809
- PMCID: PMC3558235
- DOI: 10.1016/j.jus.2011.01.006
Carpal tunnel: Normal anatomy, anatomical variants and ultrasound technique
Abstract
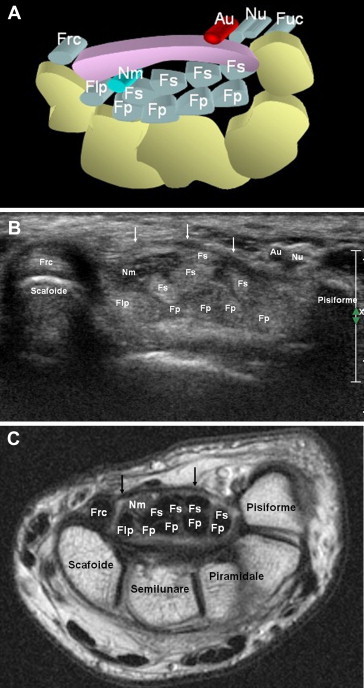
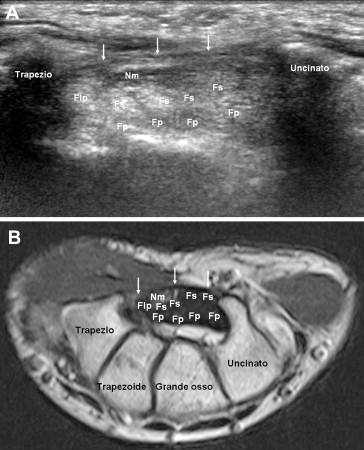
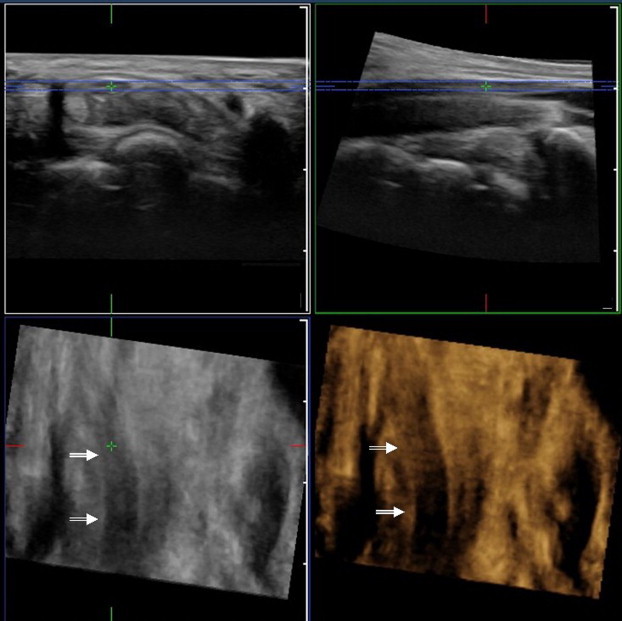
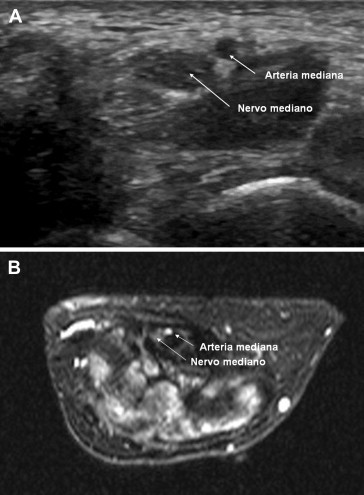
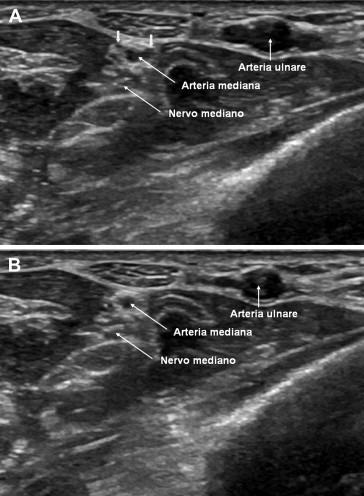
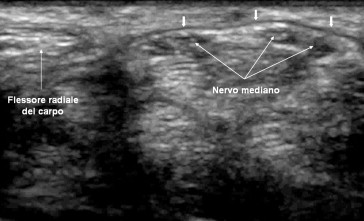
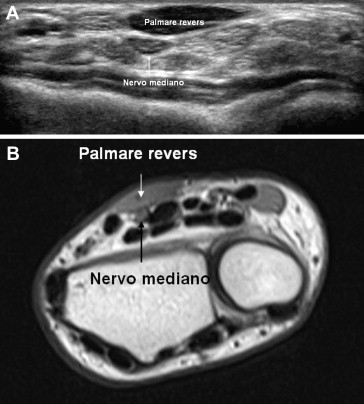
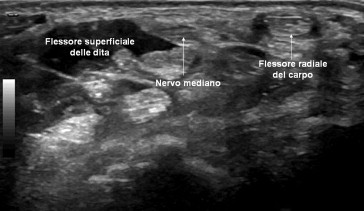
The carpal tunnel is an osteofibrous canal situated in the volar wrist. The boundaries are the carpal bones and the flexor retinaculum. In addition to the medial nerve, the carpal tunnel contains nine tendons: the flexor pollicis longus, the four flexor digitorum superficialis and the four flexor digitorum profundus. Ultrasound (US) study of the carpal tunnel generally involves short-axis imaging of the tendons, and in the presence of disease, long-axis imaging and dynamic maneuvers are added. There are numerous reports of anatomical variants of the wrist involving vessels, nerves, tendons and muscles, and they can all be studied by US. Some are particularly relevant from a clinical point of view and will therefore be accurately described. The anatomy is complex, and the US operator should therefore be thoroughly familiar with the normal anatomy as well as the anatomical variants that may have a role in the pathogenesis of carpal tunnel syndrome or influence treatment.
SommarioIl tunnel carpale è un canale osteo-fibroso localizzato nella regione volare del polso, delimitato profondamente, medialmente e lateralmente dalle ossa del carpo e superficialmente dal retinacolo dei flessori.Al suo interno decorrono nove tendini: il flessore lungo del pollice, i quattro flessori superficiali delle dita, i quattro flessori profondi delle dita ed un nervo, il mediano.Lo studio ecografico del tunnel carpale avviene generalmente per asse corto rispetto ai tendini ed è completato, almeno in presenza di patologia, da scansioni per asse lungo e manovre dinamiche.A livello del polso esistono poi numerose varianti anatomiche coinvolgenti vasi, nervi, tendini e muscoli, tutte ben valutabili ecograficamente. Alcune hanno una maggior rilevanza clinica e sono pertanto oggetto di una descrizione più accurata.L’anatomia normale è complessa, ma la sua conoscenza è essenziale per lo studio della patologia, come è essenziale la conoscenza delle varianti anatomiche che possono avere un ruolo nella patogenesi della sindrome del tunnel carpale o condizionarne le terapie.
Keywords: Carpal tunnel; Flexor tendons; Median nerve; Ultrasound.
Figures


References
-
- Martinoli C., Bianchi S., Gandolfo N., Valle M., Simonetti S., Derchi L.E. US of nerve entrapments in osteofibrous tunnels of the upper and lower limbs. RadioGraphics. 2000;20:S199–S217. - PubMed
-
- Lee J.C., Healy J.C. Normal sonographic anatomy of the wrist and hand. RadioGraphics. 2005;25:1577–1590. - PubMed
-
- Adani R., Leo G., Tarallo L., Marcoccio I., Fregni U. Il trattamento dei neurinomi dolorosi del ramo sensitivo del nervo radiale. Riv Chir Mano. 2005;42(3):127–134.
LinkOut - more resources
Full Text Sources