

Adenosine A1 receptor activation attenuates lung ischemia-reperfusion injury
- PMID: 23398646
- PMCID: PMC3657333
- DOI: 10.1016/j.jtcvs.2013.01.006
Adenosine A1 receptor activation attenuates lung ischemia-reperfusion injury
Abstract
Objectives: Ischemia-reperfusion injury contributes significantly to morbidity and mortality in lung transplant patients. Currently, no therapeutic agents are clinically available to prevent ischemia-reperfusion injury, and treatment strategies are limited to maintaining oxygenation and lung function. Adenosine can modulate inflammatory activity and injury by binding to various adenosine receptors; however, the role of the adenosine A1 receptor in ischemia-reperfusion injury and inflammation is not well understood. The present study tested the hypothesis that selective, exogenous activation of the A1 receptor would be anti-inflammatory and attenuate lung ischemia-reperfusion injury.
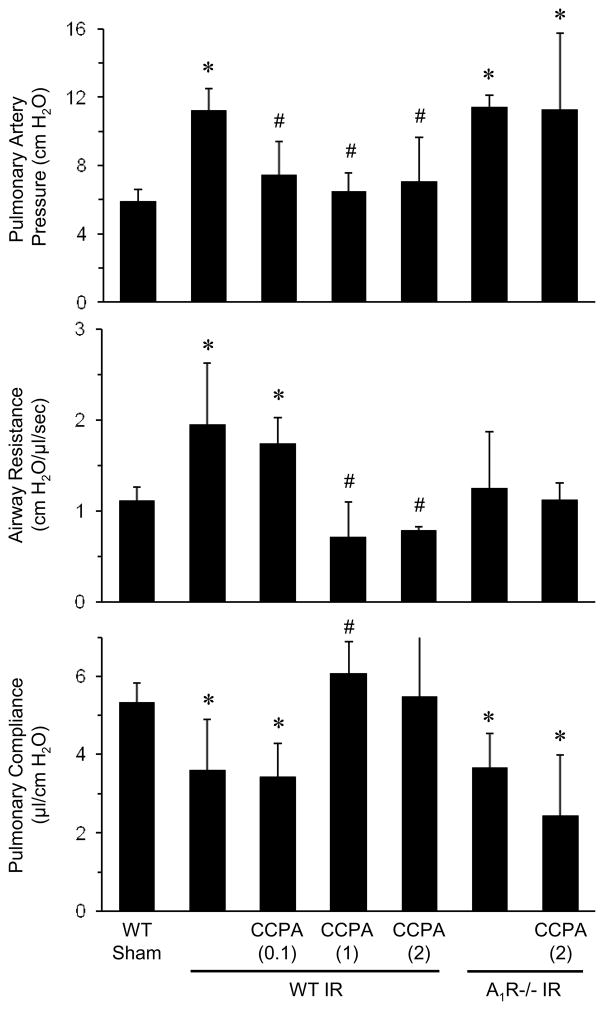
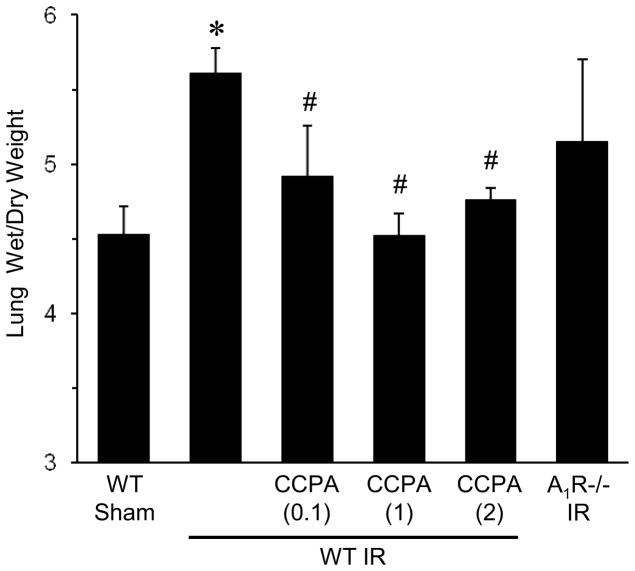
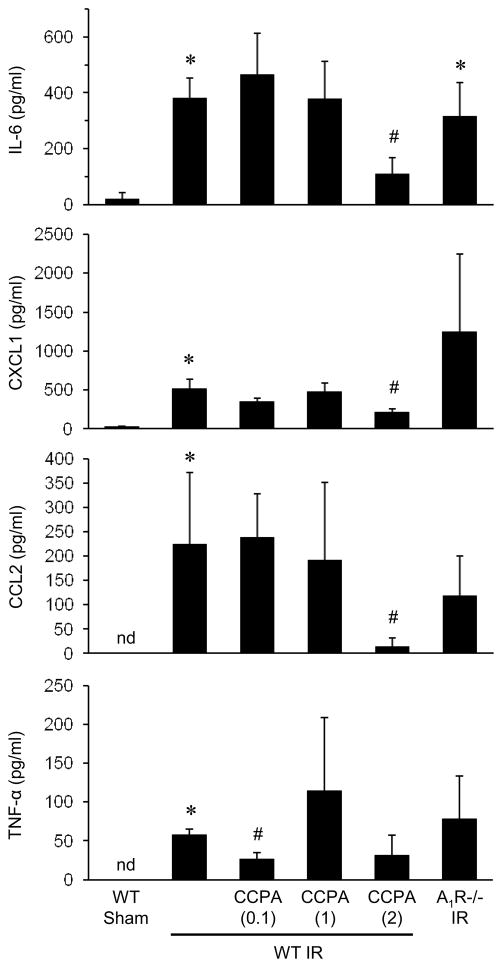
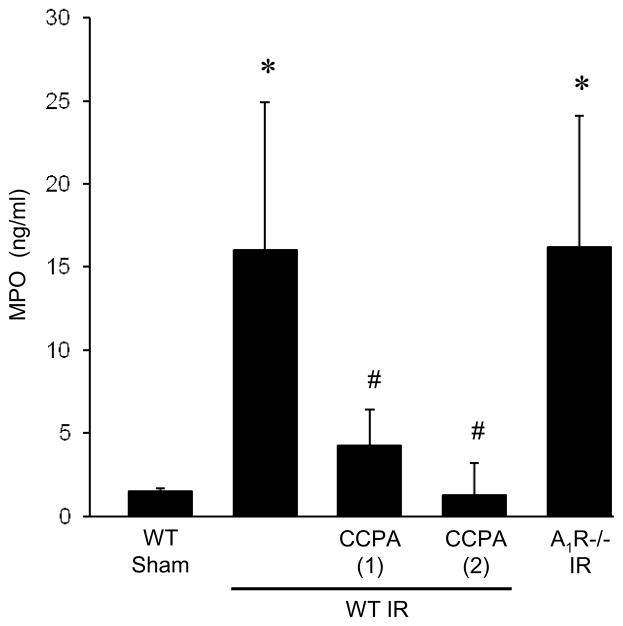
Methods: Wild-type and A1 receptor knockout mice underwent 1 hour of left lung ischemia and 2 hours of reperfusion using an in vivo hilar clamp model. An A1 receptor agonist, 2-chloro-N6-cyclopentyladenosine, was administered 5 minutes before ischemia. After reperfusion, lung function was evaluated by measuring airway resistance, pulmonary compliance, and pulmonary artery pressure. The wet/dry weight ratio was used to assess edema. The myeloperoxidase and cytokine levels in bronchoalveolar lavage fluid were measured to determine the presence of neutrophil infiltration and inflammation.
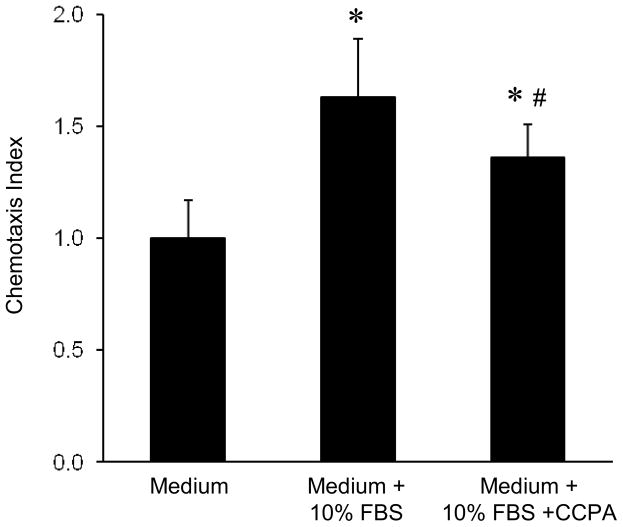
Results: In the wild-type mice, 2-chloro-N6-cyclopentyladenosine significantly improved lung function and attenuated edema, cytokine expression, and myeloperoxidase levels compared with the vehicle-treated mice after ischemia-reperfusion. The incidence of lung ischemia-reperfusion injury was similar in the A1 receptor knockout and wild-type mice; and 2-chloro-N6-cyclopentyladenosine had no effects in the A1 receptor knockout mice. In vitro treatment of neutrophils with 2-chloro-N6-cyclopentyladenosine significantly reduced chemotaxis.
Conclusions: Exogenous A1 receptor activation improves lung function and decreases inflammation, edema, and neutrophil chemotaxis after ischemia and reperfusion. These results suggest a potential therapeutic application for A1 receptor agonists for the prevention of lung ischemia-reperfusion injury after transplantation.
Copyright © 2013 The American Association for Thoracic Surgery. Published by Mosby, Inc. All rights reserved.
Conflict of interest statement
All authors declare that they have no conflict of interests.
Figures
References
-
- den Hengst WA, Gielis JF, Lin JY, Van Schil PE, De Windt LJ, Moens AL. Lung ischemia-reperfusion injury: a molecular and clinical view on a complex pathophysiological process. Am J Physiol Heart Circ Physiol. 2010;299:H1283–99. - PubMed
-
- Fan M, Qin W, Mustafa SJ. Characterization of adenosine receptor(s) involved in adenosine-induced bronchoconstriction in an allergic mouse model. Am J Physiol Lung Cell Mol Physiol. 2003;284:L1012–9. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
