

Revisiting the white blood cell count: immature granulocytes count as a diagnostic marker to discriminate between SIRS and sepsis--a prospective, observational study
- PMID: 23398965
- PMCID: PMC3575223
- DOI: 10.1186/1471-2172-14-8
Revisiting the white blood cell count: immature granulocytes count as a diagnostic marker to discriminate between SIRS and sepsis--a prospective, observational study
Abstract
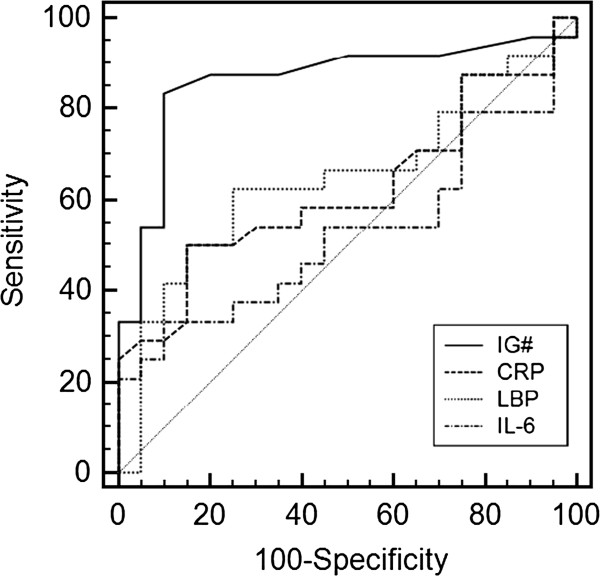
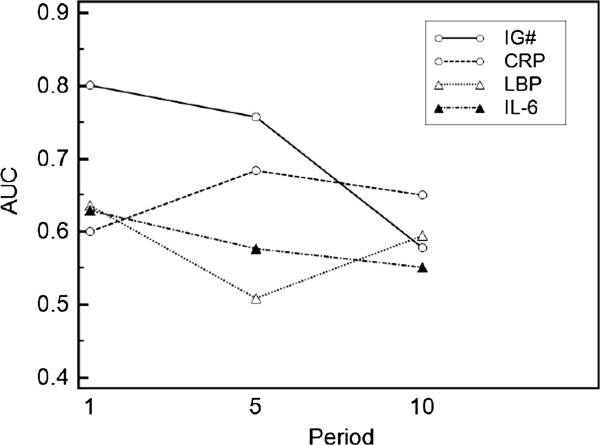
Background: Sepsis is a serious disease condition and a major cause of intensive care unit (ICU) admission. Its diagnosis in critically ill patients is complicated. To diagnose an infection rapidly, and to accurately differentiate systemic inflammatory response syndrome (SIRS) from sepsis, is challenging yet early diagnosis is vital for early induction of an appropriate therapy. The aim of this study was to evaluate whether the immature granulocyte (IG) count is a useful early diagnostic marker of sepsis compared to other markers. Therefore, a total of 70 consecutive surgical intensive care patients were assessed. IGs were measured from whole blood samples using an automated analyzer. C-reactive protein (CRP), lipopolysaccharide binding protein (LBP) and interleukin-6 (IL-6) concentrations were also determined. The observation period was a maximum of 21 days and ended with the patients' discharge from ICU or death. Receiver operating characteristic (ROC) analyses were conducted and area under the curve (AUC) was calculated to determine sensitivities and specificities for the parameters.
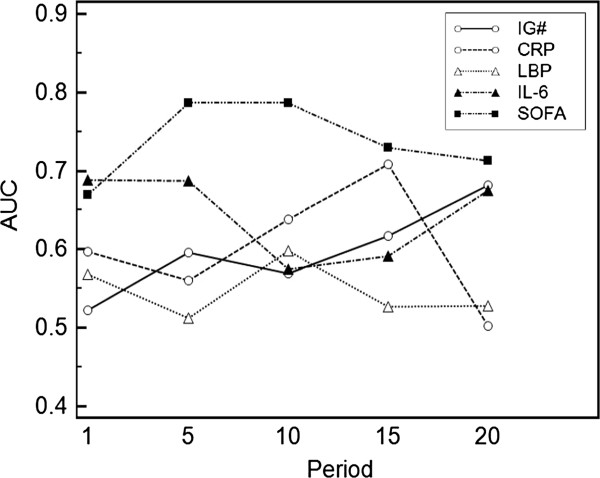
Results: We found that the IG count significantly discriminates between infected and non-infected patients (P < 0.0001) with a sensitivity of 89.2% and a specificity of 76.4%, particularly within the first 48 hours after SIRS onset. Regarding the discriminative power for infection, the IG count was more indicative than other clinical parameters such as CRP, LBP and IL-6, which had a sensitivity of less than 68%. Additionally, the highest diagnostic odds ratio (DOR) with 26.7 was calculated for the IG count within the first 48 hours. During the course of the disease ROC curve analyses showed a superior positive predictive value of the IG count compared to the other measured parameters during the first five days following the fulfillment of SIRS criteria. However, the number of IGs was not correlated with ICU mortality.
Conclusions: The total number of IG in peripheral blood from ICU patients is a good marker to discriminate infected and non-infected patients very early during SIRS. However, the IG count is not suitable as a prognostic marker for mortality. Routine and serial measurement of IGs may provide new possibilities for rapid screening of SIRS patients on ICU with suspected infections.
Figures
References
-
- Bone RC, Balk RA, Cerra FB, Dellinger RP, Fein AM, Knaus WA, Schein RM, Sibbald WJ. Definitions for sepsis and organ failure and guidelines for the use of innovative therapies in sepsis. The ACCP/SCCM consensus conference committee. American college of chest physicians/society of critical care medicine. Chest. 1992;101(6):1644–1655. doi: 10.1378/chest.101.6.1644. - DOI - PubMed
-
- Levy MM, Fink MP, Marshall JC, Abraham E, Angus D, Cook D, Cohen J, Opal SM, Vincent JL, Ramsay G. SCCM/ESICM/ACCP/ATS/SIS international sepsis definitions conference. Intensive Care Med. 2001;29(4):530–538. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
