

Looking for predictive factors of clinical response to adsorptive granulocyte and monocyte apheresis in patients with ulcerative colitis: markers of response to GMA
- PMID: 23399416
- PMCID: PMC3583683
- DOI: 10.1186/1471-230X-13-27
Looking for predictive factors of clinical response to adsorptive granulocyte and monocyte apheresis in patients with ulcerative colitis: markers of response to GMA
Abstract
Background: Adsorptive granulocyte and monocyte apheresis (GMA) with an Adacolumn in patients with ulcerative colitis (UC) has been applied as a non-pharmacological treatment strategy, but the efficacy has been encouraging as well as discouraging, depending on patients' demography at entry. In this study, we looked for predictive factors for clinical response to GMA in patients with UC.
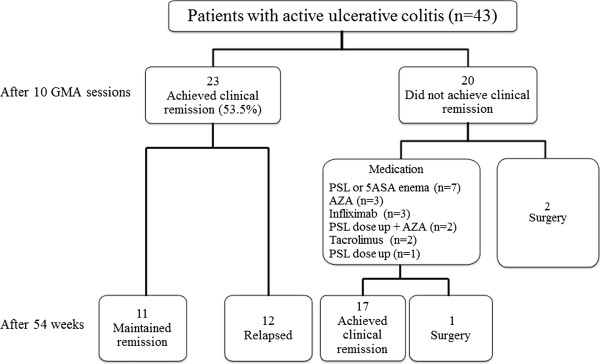
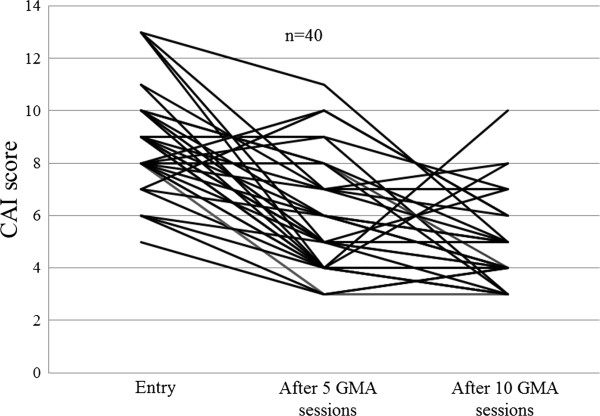
Methods: In a retrospective setting, 43 outpatients who had been treated with GMA for active UC were evaluated. Patients were divided into remission group and non-remission group based on Lichtiger's clinical activity index (CAI) before and after 10, once a week GMA sessions. The efficacy was analysed in relation to patients' demographic variables. To determine predictive factors that closely related to the response to GMA, receiver operating characteristic (ROC) curve, and multiple logistic regression analyses were applied.
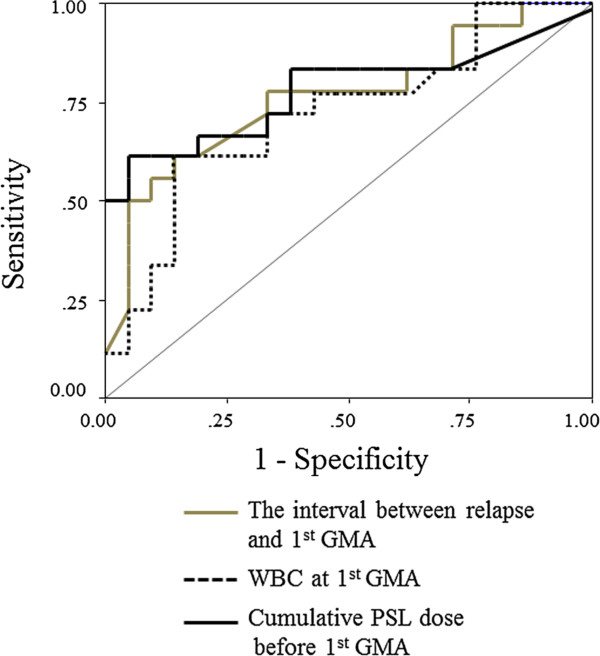
Results: After 10 GMA sessions, the overall clinical remission rate (CAI < 4) was 53.5%. Multiple logistic regression and ROC analyses showed that the interval between relapse and the first GMA session was a significant and independent predictive factor for clinical response to GMA (P = 0.016); the clinical response was better in patients who received GMA immediately after a relapse and vice versa. Likewise, univariate analyses showed that, the duration of UC (P = 0.036) and the cumulative prednisolone (PSL) dose (P = 0.006) before the first GMA session were significantly greater in the GMA non-responder group as compared with the responder group. Additionally, a lower white blood cell (WBC) count at first GMA session was related to clinical response to GMA (P = 0.032).
Conclusions: In this study, patients with a short duration of UC and low cumulative PSL dose seemed to respond well to GMA. However, we found that the best responders were patients who received GMA immediately after a clinical relapse. Additionally, GMA was effective in patients with low WBC count at the first GMA session. The findings of this study should spare medical cost and reduce morbidity time for many patients, relevant for decision making in clinical settings.
Figures
References
-
- Allison MC, Dhillon AP, Lewis WG, Pounder RE. Inflammatory Bowel Disease. London: Mosby; 1998. pp. 9–95.
-
- Yokoyama Y, Fukunaga K, Fukuda Y, Tozawa K, Kamikozuru K, Ohnishi K, Kusaka T, Kosaka T, Hida N, Ohda Y, Miwa H, Matsumoto T. Demonstration of low-regulatory CD25HighCD4+ and high-pro-inflammatory CD28-CD4+ T-Cell subsets in patients with ulcerative colitis: modified by selective granulocyte and monocyte adsorption apheresis. Dig Dis Sci. 2007;52:2725–2731. doi: 10.1007/s10620-006-9560-z. - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
