

Patient mobility for cardiac problems: a risk-adjusted analysis in Italy
- PMID: 23399540
- PMCID: PMC3606354
- DOI: 10.1186/1472-6963-13-56
Patient mobility for cardiac problems: a risk-adjusted analysis in Italy
Abstract
Background: The Italian National Health System was revised in the last 20 years, introducing new elements such as efficacy, efficiency and competitiveness. Devolution to regional authorities has created a quasi-market system where patients can choose the hospital in which to be treated. Patient mobility therefore becomes an indicator of perceived hospital quality and of financial flows between the regions of Italy. Previous studies analyzed patient mobility in general or by specific disease/diagnosis-related groups but there is a lack of research on the influence of severity of patient condition. The aim of the study was to describe patient mobility, crude and stratified by disease severity, in cardiac surgery units of three health areas (HAs) in Tuscany (Italy).
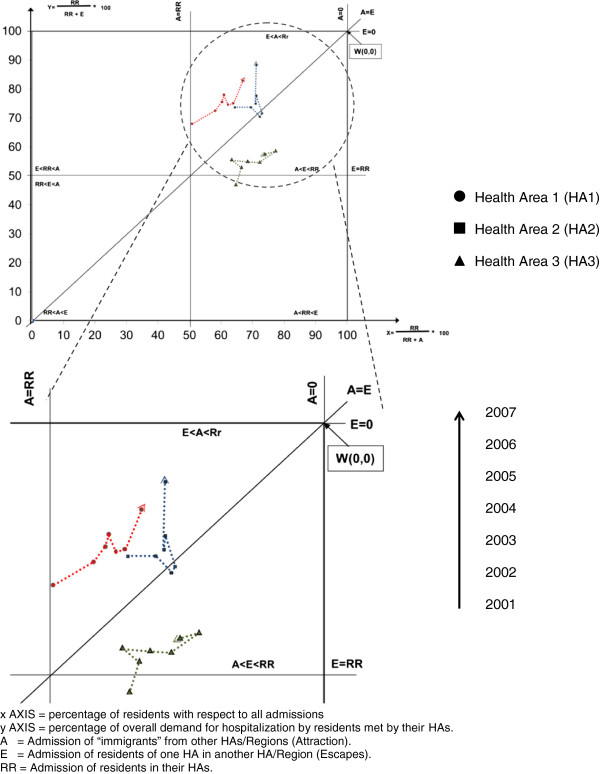
Methods: In this retrospective observational study, data was gathered from hospital discharge records obtained from the Tuscan Regional Health Agency, Italy. The three HAs (HA1, HA2, HA3) recorded 25,017 planned hospitalizations in cardiac surgery units in the period 2001-2007. Patients were stratified in four All Patient Refined Diagnosis Related Group (APR-DRG) severity levels. Gandy's nomogram was used to describe how HAs met health care demand and their capacity to attract patients. Cuzick's test was used to identify significant differences in time trends.
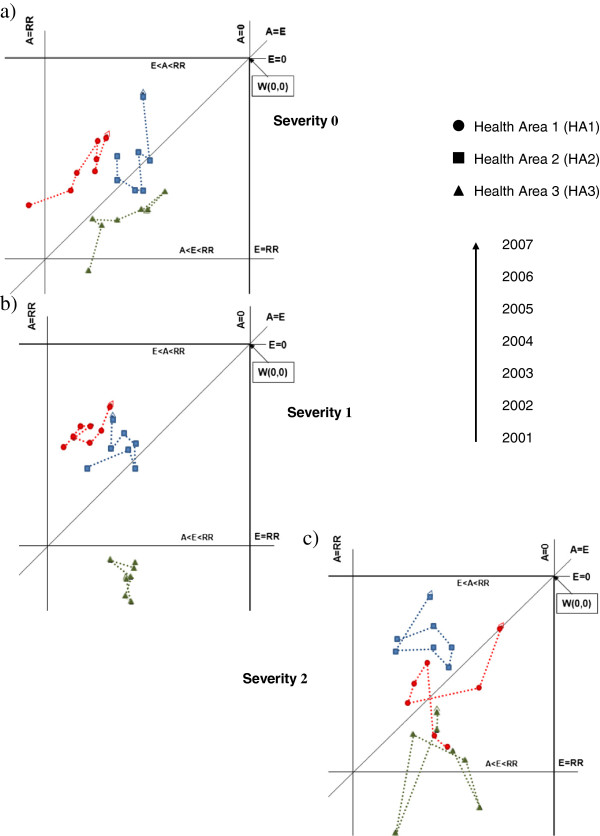
Results: Raw data showed that the HAs met their own local health care demand. Stratifying by APR-DRG severity, it emerged that capacity to meet local demand remained unchanged for zero-to-minor severity levels, but one HA was less able to meet demand for moderate severity levels or to attract patients from other HAs and Regions of Italy. In fact, HA3 showed a decrease in admissions of local residents.
Conclusions: The study highlights important differences between the three HAs that were only revealed by severity stratification: unlike HA3, HA1 and HA2 seemed able to deal with local demand, even after severity stratification. Planners and researchers can benefit from risk stratification data, which provides more elements for correct comparisons and interventions. In the context of patient mobility, the present study is a step in that direction.
Figures
References
-
- Donabedian A. Evaluating the quality of medical care. Milbank Q. 1966;44(3):166–206. - PubMed
-
- Messina G, Vigiani N, Lispi L, Nante N. Patient migration among the Italian regions 2003. Italian Journal Of Public Health. 2008;5(1):45–52.
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
