

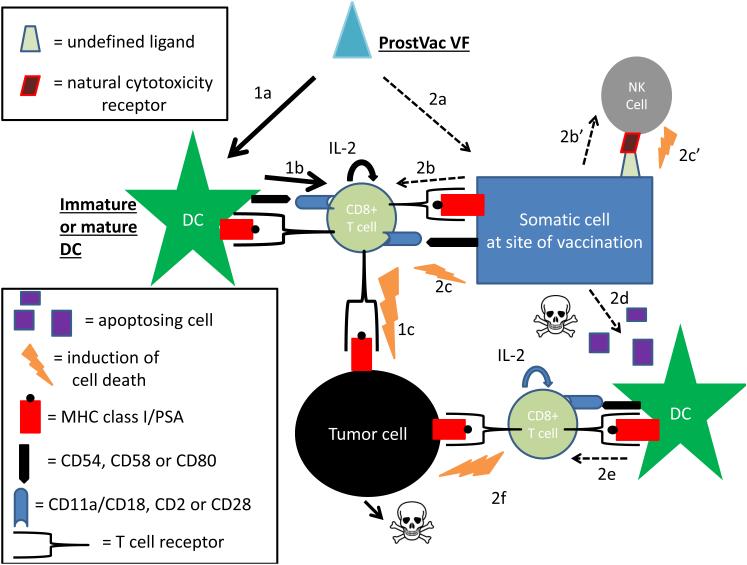
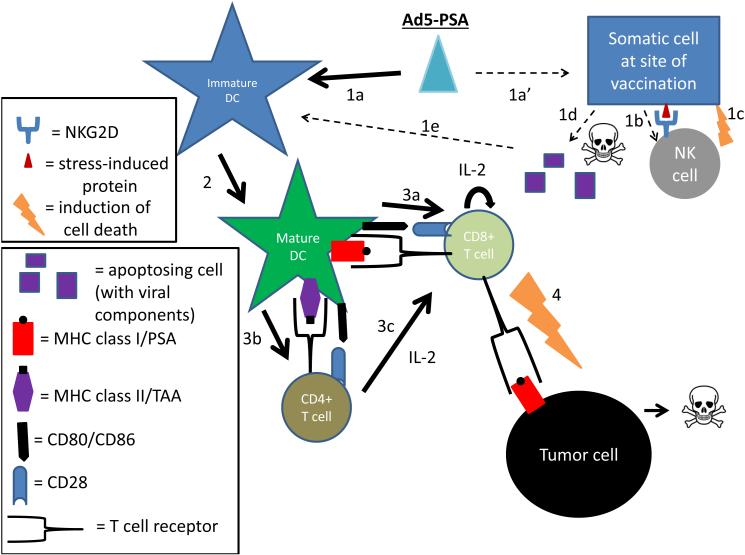
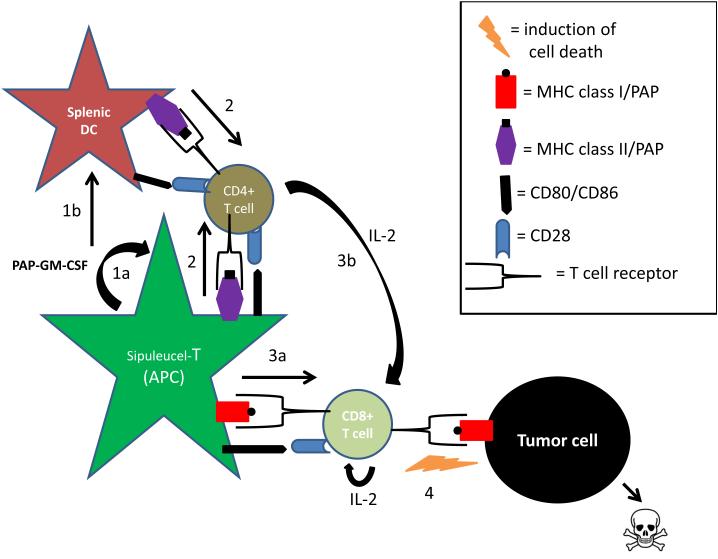
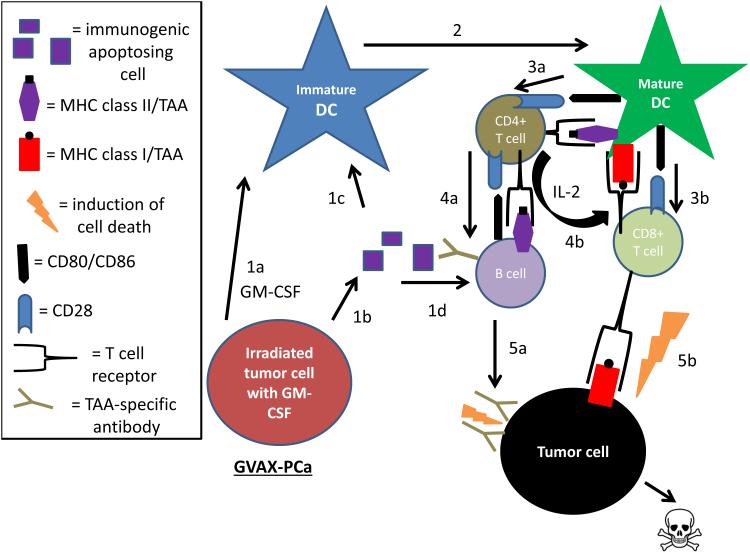
Proposed mechanisms of action for prostate cancer vaccines
- PMID: 23399727
- PMCID: PMC4358823
- DOI: 10.1038/nrurol.2013.8
Proposed mechanisms of action for prostate cancer vaccines
Abstract
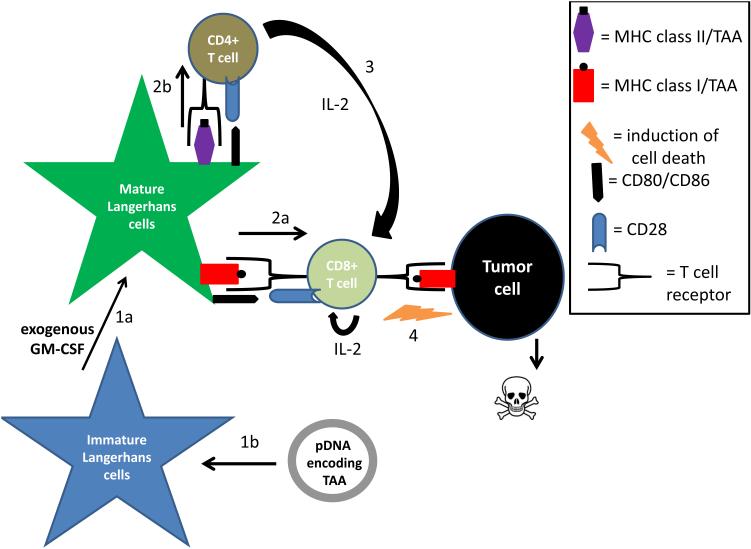
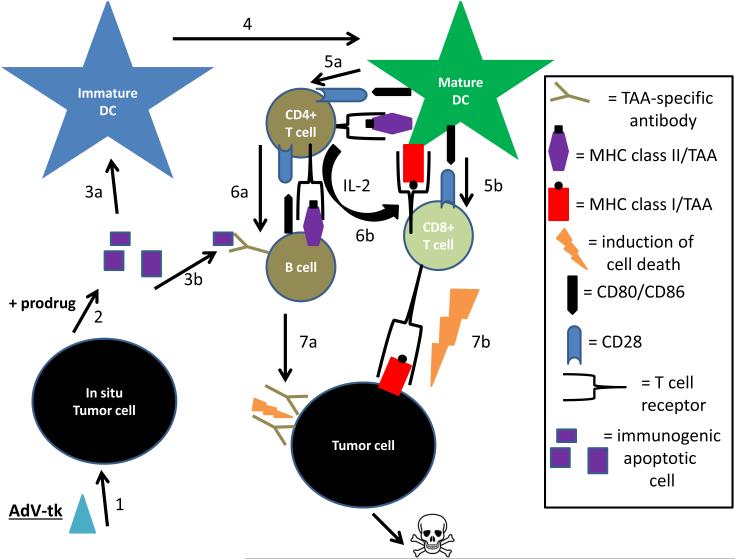
Prostate cancer is responsible for the deaths of more than 33,000 American men every year. Once this disease has become metastatic, there is no curative treatment. Alternative therapies to chemotherapy and radical prostatectomy are being increasingly explored. Prostate cancer vaccines--which trigger a tumour-specific cytotoxic-T-lymphocyte-mediated immune attack by the patient's immune system--have been investigated in clinical trials with modest, yet encouraging, results. When developing and administering prostate cancer vaccines, it is critical to consider how vital parameters, such as the stage of disease progression and the nature of adjuvant therapies, could influence treatment outcome. Of particular interest are current and future strategies for diminishing the activity of regulatory T lymphocytes.
Figures
References
-
- Siegel R, Naishadham D, Jemal A. Cancer statistics, 2012. CA Cancer J Clin. 2012;62:10–29. - PubMed
-
- Pound CR, et al. Natural history of progression after PSA elevation following radical prostatectomy. JAMA. 1999;281:1591–1597. - PubMed
-
- Beltran H, et al. New therapies for castration-resistant prostate cancer: efficacy and safety. Eur Urol. 2011;60:279–290. - PubMed
-
- Karan D, Holzbeierlein JM, Van Veldhuizen P, Thrasher JB. Cancer immunotherapy: a paradigm shift for prostate cancer treatment. Nat Rev Urol. 2012;9:376–385. - PubMed
-
- Kantoff PW, et al. Sipuleucel-T immunotherapy for castration-resistant prostate cancer. N Engl J Med. 2010;363:411–422. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
