

Onlay ventral hernia repairs using porcine non-cross-linked dermal biologic mesh
- PMID: 23400527
- PMCID: PMC4177570
- DOI: 10.1007/s10029-013-1054-2
Onlay ventral hernia repairs using porcine non-cross-linked dermal biologic mesh
Abstract
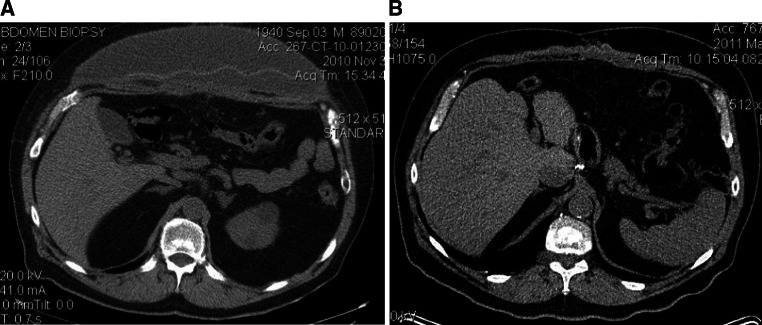
Introduction: Ventral hernias are common and repair with mesh has been shown to reduce recurrence. However, synthetic mesh is associated with a risk of infection. Biologic mesh is an alternative that may be less susceptible to infection. Typically, the sublay position is preferred for mesh placement but this technique takes longer and has not been shown to have a lower recurrence rate than an onlay mesh. The aim of this study was to evaluate the outcome of complex ventral hernia repair using a porcine non-cross-linked biologic mesh onlay.
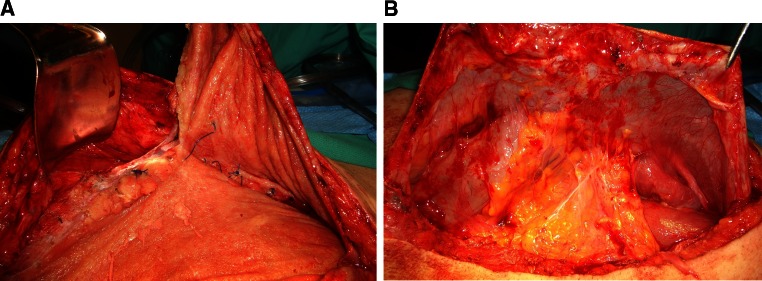
Methods: A retrospective chart review was performed of all patients that had a ventral hernia repair with biologic mesh from January 2009 to March 2012. The operative procedure in all patients was an open repair with primary fascial closure (if possible) with or without external oblique component separation and porcine biologic mesh onlay.
Results: There were 22 patients that had a ventral hernia repair, 19 primary and 3 recurrent. The majority were men, had hernia grade 3 or 4, and developed the hernia after an esophagectomy or gastrectomy for cancer. All but one had primary closure with a porcine biologic mesh onlay. One patient was bridged for loss of domain. A bilateral external oblique component separation was added in 16 patients (73 %). The median hospital stay was 7 days. There were two superficial wound infections, one with exposed mesh, but no patient required mesh removal. A seroma requiring intervention developed in 6 patients (27 %) and resolved with pig-tail drainage. At a median follow-up of 7 months, there has been no hernia recurrence apart from the patient that was bridged.
Conclusions: Porcine non-cross-linked biologic mesh overlay has excellent short-term results in patients at increased risk for mesh infection. No patient required mesh removal, and there have been no recurrent hernias in patients with primary fascial closure. Biologic bridging is not effective for long-term abdominal wall reconstruction.
Figures



References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
