

Cost-effectiveness of the School-Based Asthma Therapy (SBAT) program
- PMID: 23400614
- PMCID: PMC3581846
- DOI: 10.1542/peds.2012-1883
Cost-effectiveness of the School-Based Asthma Therapy (SBAT) program
Abstract
Background and objective: Impoverished urban children suffer disproportionately from asthma and underuse preventive asthma medications. The objective of this study was to examine cost-effectiveness (CE) of the School-Based Asthma Therapy (SBAT) program compared with usual care (UC).
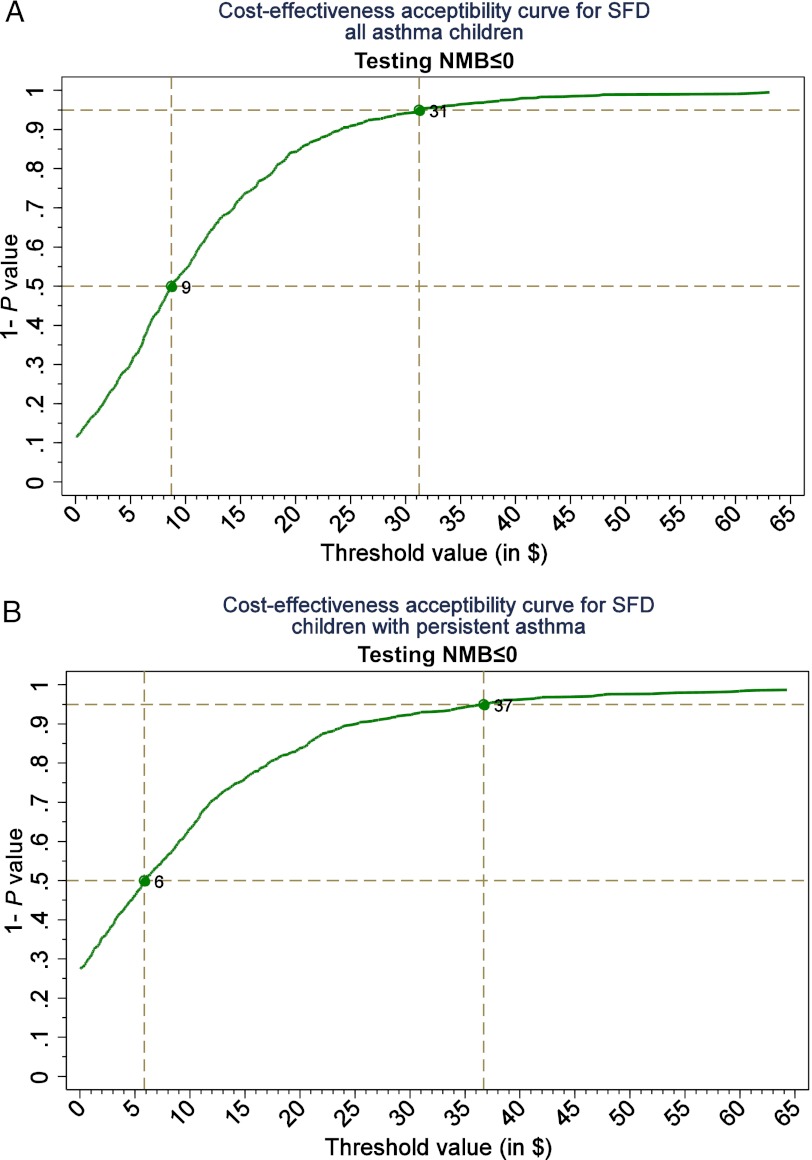
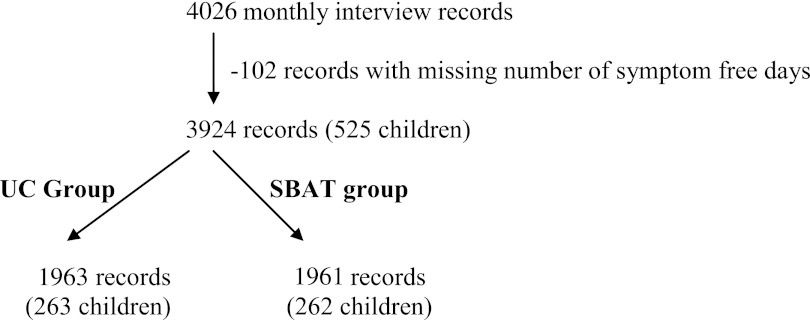
Methods: The analysis was based on the SBAT trial, including 525 children aged 3 to 10 years attending urban preschool or elementary school who were randomized to either UC or administration of 1 dose of preventive asthma medication at school by the school nurse each school day. The primary outcome was the mean number of symptom-free days (SFDs). The impact of the intervention on medical costs was estimated by using parent-reported child health services utilization data and average national reimbursement rates. We estimated the cost of running the program using wages for program staff. Productivity costs were estimated by using value of parent lost time due to child illness. CE of the SBAT program compared with UC was evaluated based on the incremental CE ratio.
Results: The health benefit of the intervention was equal to ∼158 SFD gained per each 30-day period (P < .05) per 100 children. The programmatic expenses summed to an extra $4822 per 100 children per month. The net saving due to the intervention (reduction in medical costs and parental productivity, and improvement in school attendance) was $3240, resulting in the incremental cost-savings difference of $1583 and CE of $10 per 1 extra SFD gained.
Conclusions: The SBAT was effective and cost-effective in reducing symptoms in urban children with asthma compared with other existing programs.
Trial registration: ClinicalTrials.gov NCT01175369.
Figures
Comment in
-
School-based asthma controller medication administration is associated with cost savings.J Pediatr. 2013 Jul;163(1):304. doi: 10.1016/j.jpeds.2013.04.061. J Pediatr. 2013. PMID: 23796345 No abstract available.
References
-
- Adams PF, Marano MA. Current estimates from the National Health Interview Survey, 1994. Vital Health Stat 10. 1995;(193 pt 1):1–260 - PubMed
-
- Centers for Disease Control and Prevention. Surveillance for asthma—US, 1960–1995. CDC Surveillance Summaries. 1995;47:1022–1025
-
- National Heart Laboratory. Data Fact Sheet. Asthma Statistics. Bethesda, MD: National Institutes of Health; 1999
-
- Centers for Disease Control and Prevention Asthma mortality and hospitalization among children and adults—United States, 1980–1993. MMWR Morb Mortal Wkly Rep. 1996;45(17):350–353 - PubMed
-
- Gergen PJ, Weiss KB. Changing patterns of asthma hospitalization among children: 1979 to 1987. JAMA. 1990;264(13):1688–1692 - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
