

Computed tomography screening for lung cancer: has it finally arrived? Implications of the national lung screening trial
- PMID: 23401434
- PMCID: PMC3589698
- DOI: 10.1200/JCO.2012.43.3110
Computed tomography screening for lung cancer: has it finally arrived? Implications of the national lung screening trial
Abstract
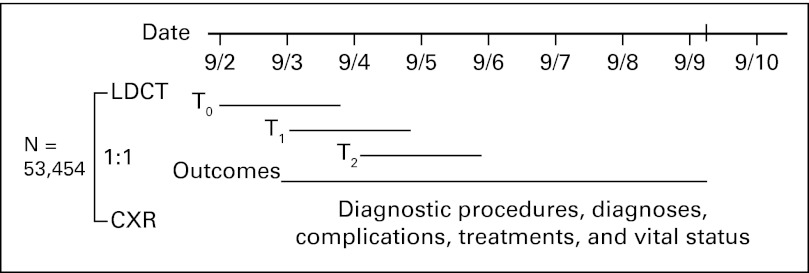
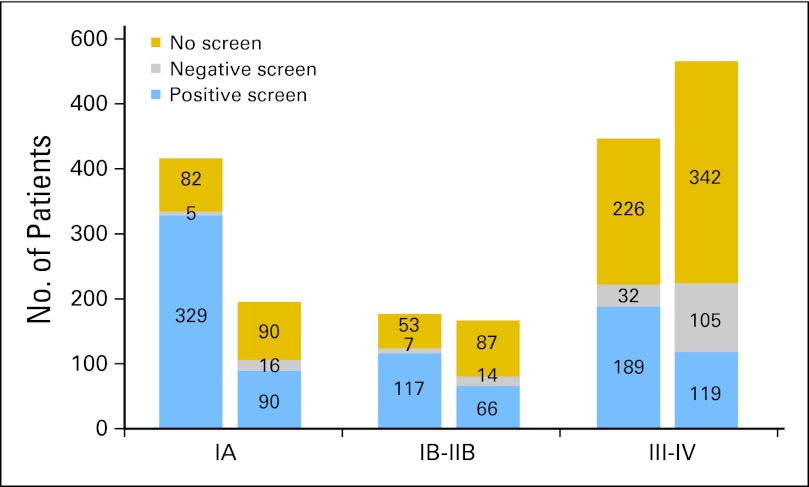
The National Lung Screening Trial (NLST) has provided compelling evidence of the efficacy of lung cancer screening using low-dose helical computed tomography (LDCT) to reduce lung cancer mortality. The NLST randomized 53,454 older current or former heavy smokers to receive LDCT or chest radiography (CXR) for three annual screens. Participants were observed for a median of 6.5 years for outcomes. Vital status was available in more than 95% of participants. LDCT was positive in 24.2% of screens, compared with 6.9% of CXRs; more than 95% of all positive LDCT screens were not associated with lung cancer. LDCT detected more than twice the number of early-stage lung cancers and resulted in a stage shift from advanced to early-stage disease. Complications of LDCT screening were minimal. Lung cancer-specific mortality was reduced by 20% relative to CXR; all-cause mortality was reduced by 6.7%. The major harms of LDCT are radiation exposure, high false-positive rates, and the potential for overdiagnosis. This review discusses the risks and benefits of LDCT screening as well as an approach to LDCT implementation that incorporates systematic screening practice with smoking cessation programs and offers opportunities for better determination of appropriate risk cohorts for screening and for better diagnostic prediction of lung cancer in the setting of screen-detected nodules. The challenges of implementation are considered for screening programs, for primary care clinicians, and across socioeconomic strata. Considerations for future research to complement imaging-based screening to reduce the burden of lung cancer are discussed.
Conflict of interest statement
Authors' disclosures of potential conflicts of interest and author contributions are found at the end of this article.
Figures
References
-
- National Institutes of Health: Estimates of funding for various research, condition, and disease categories (RCDC) http://www.report.nih.gov/categorical_spending.aspx.
-
- Siegel R, Naishadham D, Jemal A. Cancer statistics, 2012. CA Cancer J Clin. 2012;62:10–29. - PubMed
-
- Melamed MR. Lung cancer screening results in the National Cancer Institute New York study. Cancer. 2000;89(suppl 11):2356–2362. - PubMed
-
- Tockman MS. Survival and mortality from lung cancer in a screened population: The Johns Hopkins Study. Chest. 1986;89(supp):324S–325S.
-
- Fontana RS, Sanderson DR, Woolner LB, et al. Screening for lung cancer: A critique of the Mayo Lung Project. Cancer. 1991;67(suppl 4):1155–1164. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
