

Theranostic nanoparticles with controlled release of gemcitabine for targeted therapy and MRI of pancreatic cancer
- PMID: 23402593
- PMCID: PMC3609912
- DOI: 10.1021/nn3043463
Theranostic nanoparticles with controlled release of gemcitabine for targeted therapy and MRI of pancreatic cancer
Abstract
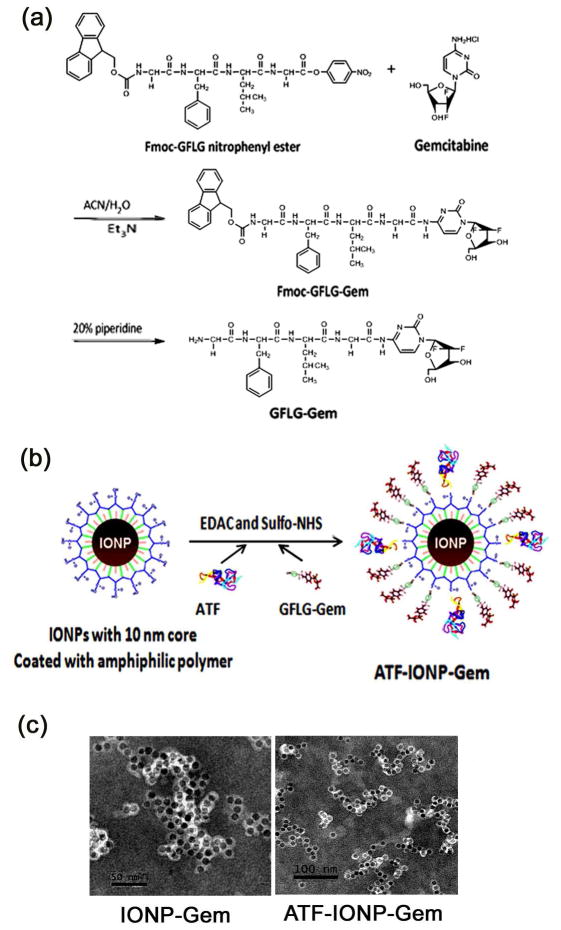
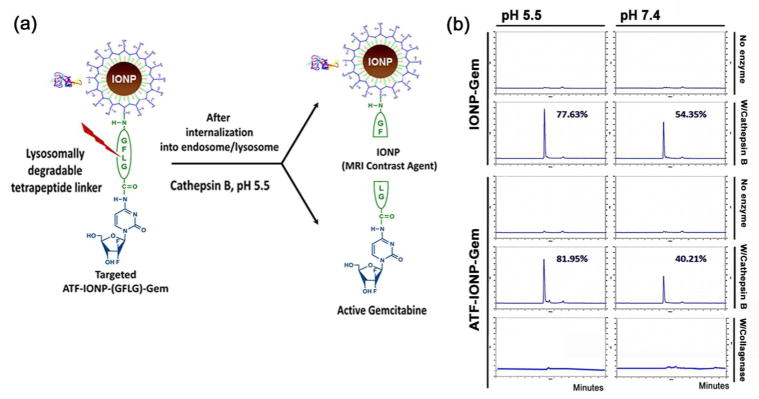
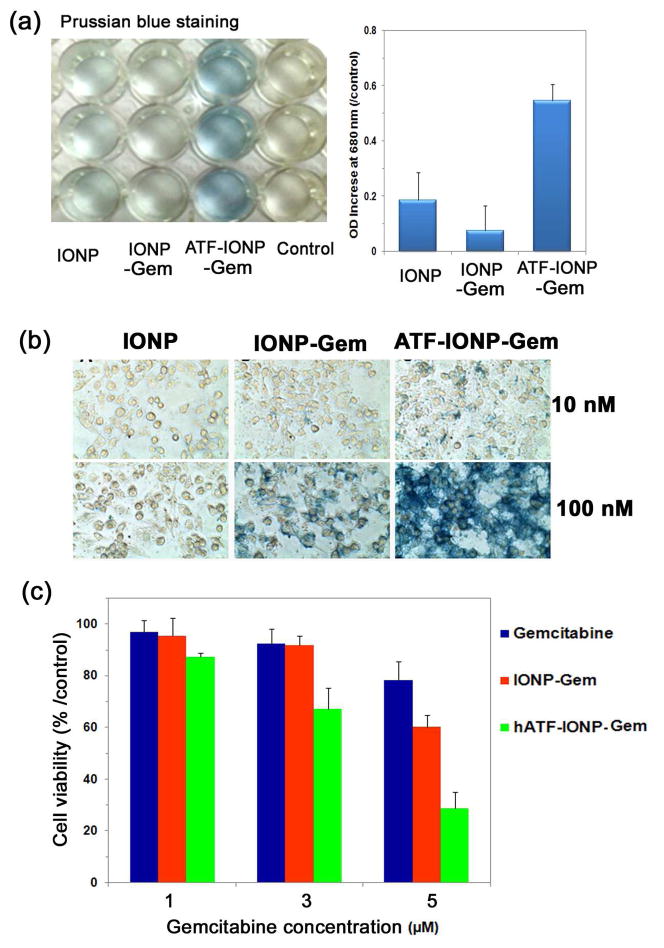
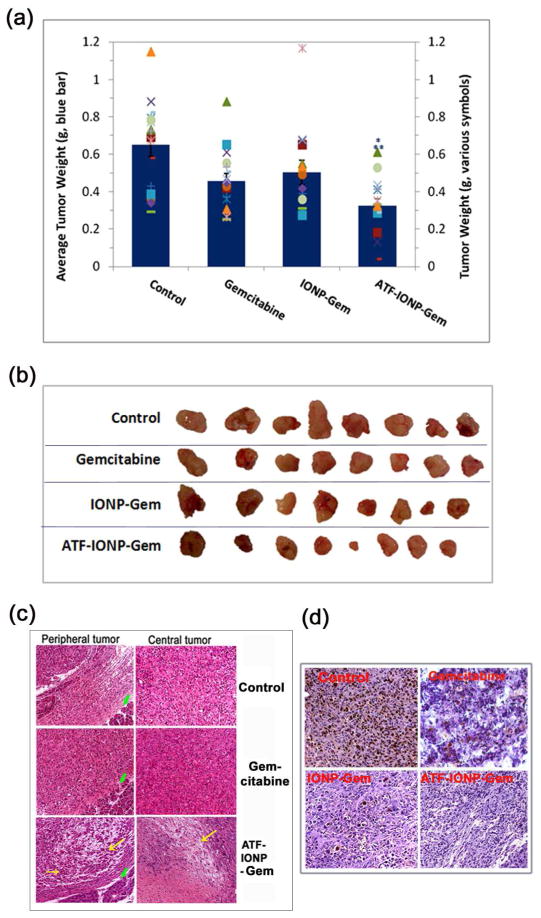
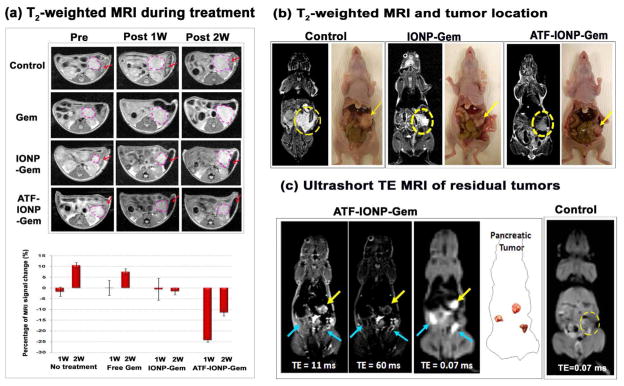
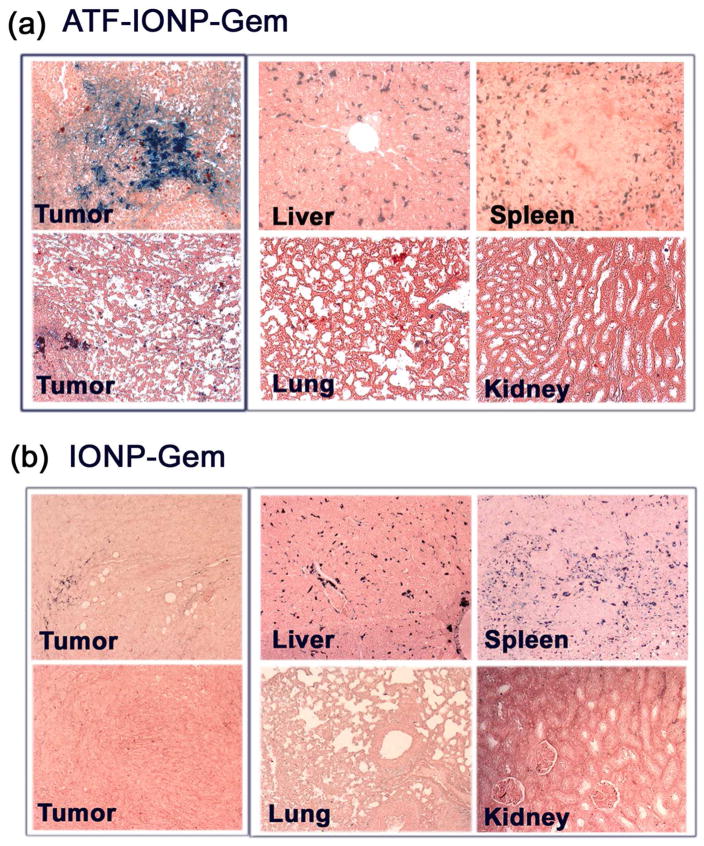
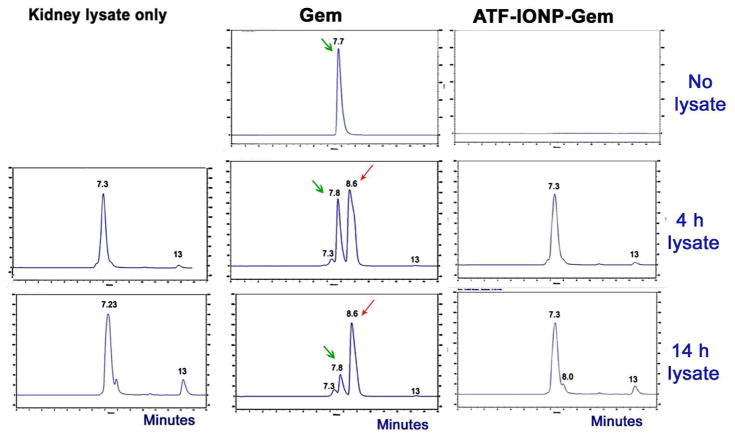
The tumor stroma in human cancers significantly limits the delivery of therapeutic agents into cancer cells. To develop an effective therapeutic approach overcoming the physical barrier of the stroma, we engineered urokinase plasminogen activator receptor (uPAR)-targeted magnetic iron oxide nanoparticles (IONPs) carrying chemotherapy drug gemcitabine (Gem) for targeted delivery into uPAR-expressing tumor and stromal cells. The uPAR-targeted nanoparticle construct, ATF-IONP-Gem, was prepared by conjugating IONPs with the amino-terminal fragment (ATF) peptide of the receptor-binding domain of uPA, a natural ligand of uPAR, and Gem via a lysosomally cleavable tetrapeptide linker. These theranostic nanoparticles enable intracellular release of Gem following receptor-mediated endocytosis of ATF-IONP-Gem into tumor cells and also provide contrast enhancement in magnetic resonance imaging (MRI) of tumors. Our results demonstrated the pH- and lysosomal enzyme-dependent release of gemcitabine, preventing the drug from enzymatic degradation. Systemic administrations of ATF-IONP-Gem significantly inhibited the growth of orthotopic human pancreatic cancer xenografts in nude mice. With MRI contrast enhancement by IONPs, we detected the presence of IONPs in the residual tumors following the treatment, suggesting the possibility of monitoring drug delivery and assessing drug-resistant tumors by MRI. The theranostic ATF-IONP-Gem nanoparticle has great potential for the development of targeted therapeutic and imaging approaches that are capable of overcoming the tumor stromal barrier, thus enhancing the therapeutic effect of nanoparticle drugs on pancreatic cancers.
Figures
References
-
- Willett CG, Czito BG, Bendell JC, Ryan DP. Locally Advanced Pancreatic Cancer. J Clin Oncol. 2005;23:4538–4544. - PubMed
-
- Warshaw AL, Fernandez-del Castillo C. Pancreatic Carcinoma. N Engl J Med. 1992;326:455–465. - PubMed
-
- Mahadevan D, Von Hoff DD. Tumor-Stroma Interactions in Pancreatic Ductal Adenocarcinoma. Mol Cancer Ther. 2007;6:1186–1197. - PubMed
-
- Kalluri R, Zeisberg M. Fibroblasts in Cancer. Nat Rev Cancer. 2006;6:392–401. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
